
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1Pharmacy Technician, CVS Pharmacy, Red Oak, Texas-75154, United States
2Associate Professor, Department of Pharmaceutics, A. M. Reddy Memorial College of Pharmacy, Petlurivaripalem, Narasaraopet, Palnadu, A.P.- India-522 601
Background: Psoriasis is a chronic, immune-mediated inflammatory skin disorder that requires long-term treatment, making medication adherence a key determinant of successful disease management. Clinical pharmacists can play an important role in enhancing treatment adherence and optimizing therapeutic outcomes. Objective: This study aimed to evaluate the prevalence of psoriasis and determine the effect of clinical pharmacist interventions on medication adherence among patients with psoriasis. Methods: A cross-sectional observational study was conducted involving 50 patients diagnosed with psoriasis. Baseline clinical and demographic data were collected, and patients were scheduled for a follow-up assessment one month after initiating treatment. Disease severity was measured using the Psoriasis Area and Severity Index (PASI), while medication adherence was assessed using the Medication Adherence Report Scale (MARS) at baseline and during the first follow-up. Results: Among the 50 enrolled patients, psoriasis severity was categorized as mild, moderate, or severe based on PASI scores. The mean baseline PASI score was 8.27 ± 5.70, which decreased to 5.43 ± 3.69 at the one-month follow-up, indicating an improvement in disease severity. The most frequently prescribed medications included cetirizine (94%), vitamin A & D preparations (78%), betamethasone cream (64%), and calcium supplements (60%). Medication adherence also improved during the study period. The mean MARS score increased from 4.74 ± 0.72 at baseline to 7.08 ± 1.31 at the first follow-up, demonstrating enhanced adherence following clinical pharmacist involvement. Conclusion: The findings suggest that clinical pharmacist interventions contribute significantly to improving medication adherence and reducing disease severity in patients with psoriasis. Strengthening the role of clinical pharmacists in patient education, counselling, and follow-up may enhance long-term therapeutic outcomes and improve the quality of care for individuals living with this chronic condition.
Psoriasis is a chronic, immune-mediated inflammatory disorder of the skin characterized by recurrent episodes of exacerbation and remission. The disease is typically manifested by well-demarcated erythematous plaques covered with silvery-white scales that may be associated with itching, pain, and discomfort. Although psoriasis primarily affects the skin, it is now recognized as a systemic inflammatory condition that can significantly impair physical, psychological, and social well-being. The visible nature of the lesions often contributes to emotional distress, reduced self-esteem, and diminished quality of life, particularly among patients with moderate to severe disease. The condition develops as a consequence of dysregulated immune responses that accelerate epidermal cell turnover, resulting in excessive proliferation and abnormal differentiation of keratinocytes [1].
Epidemiology
Psoriasis is one of the most prevalent chronic dermatological disorders worldwide, affecting individuals across different age groups and ethnic populations. In India, the reported prevalence ranges from 0.44% to 2.8%, with considerable regional variation. Hospital-based studies indicate that the disease is more frequently observed in males than females. The onset can occur at any age, although peaks are commonly seen during early adulthood and middle age [2].
Etiology
The exact cause of psoriasis has not yet been fully established. Current evidence suggests that the disease results from a complex interaction between genetic susceptibility and environmental influences, leading to immune dysregulation and chronic inflammation. In genetically predisposed individuals, various external factors may initiate or aggravate the disease process. The combined effects of these factors contribute to the development and persistence of psoriatic lesions [3].
Genetic Factors
Genetic predisposition plays a substantial role in the pathogenesis of psoriasis. Genome-wide association studies have identified multiple susceptibility loci associated with disease development. Among these, the PSORS1 locus located on chromosome 6 within the major histocompatibility complex has demonstrated the strongest association and is estimated to account for approximately 30–50% of the inherited genetic risk. Another important susceptibility region, PSORS2, has been identified on chromosome 17q. These genetic loci influence immune regulation and contribute to an increased likelihood of developing psoriasis in susceptible individuals [3].
Environmental Trigger Factors
Several environmental and lifestyle factors are known to precipitate the onset of psoriasis or worsen existing disease. Cigarette smoking, excessive alcohol consumption, psychological stress, and skin trauma are among the most frequently reported triggers. Certain medications, including lithium, β-blockers, angiotensin-converting enzyme inhibitors, antimalarial agents such as chloroquine and hydroxychloroquine, indomethacin, tetracyclines, interferons, and the abrupt withdrawal of systemic corticosteroids, have also been implicated in disease exacerbation. Infections, particularly HIV, physical injury to the skin, sunburn, and seasonal or climatic variations may further contribute to disease flare-ups in susceptible individuals [4,5].
Pathophysiology
Psoriasis is driven by a complex interplay between the innate and adaptive immune systems. Activation of dendritic cells stimulates CD4⁺ helper T cells and CD8⁺ cytotoxic T cells, resulting in an exaggerated immune response. These activated immune cells release pro-inflammatory cytokines, including tumor necrosis factor-alpha (TNF-α), interleukin (IL)-17, IL-23, and IL-22, which perpetuate chronic inflammation and promote keratinocyte hyperproliferation. The accelerated growth and impaired maturation of keratinocytes shorten the normal epidermal turnover time from approximately four weeks to only a few days, leading to the accumulation of thick, scaly plaques. Increased angiogenesis and inflammatory cell infiltration further contribute to the characteristic clinical manifestations of psoriasis [6–9].
Clinical Types and Manifestations of Psoriasis
Psoriasis presents in several clinical forms, each with distinct morphological characteristics and anatomical distribution.
Plaque psoriasis is the most common subtype and is characterized by sharply demarcated, erythematous plaques covered with silvery-white scales. These lesions most frequently occur on the scalp, elbows, knees, and lower back and are often accompanied by itching or pain [10,11].
Guttate psoriasis is characterized by numerous small, drop-shaped papules measuring approximately 1–10 mm in diameter. It commonly affects the trunk and proximal limbs and frequently develops following streptococcal throat infections [12,13].
Inverse psoriasis primarily involves intertriginous regions such as the axillae, groin, inframammary folds, and other skin folds. Lesions appear as smooth, erythematous patches with minimal scaling because of the moist environment of these areas [14].
Pustular psoriasis is an uncommon but severe form characterized by sterile, pus-filled pustules surrounded by erythematous skin. It may be localized to the palms and soles or become generalized, requiring urgent medical attention [15].
Erythrodermic psoriasis represents a rare and potentially life-threatening variant involving diffuse erythema, extensive scaling, severe inflammation, and systemic manifestations affecting most of the body surface area [16].
Nail psoriasis affects the fingernails and toenails, producing pitting, discoloration, subungual hyperkeratosis, nail thickening, and onycholysis, which may impair hand function and quality of life [17].
Scalp psoriasis presents with well-defined erythematous plaques covered by thick scales on the scalp and is commonly associated with persistent itching and irritation [18].
Palmoplantar psoriasis involves the palms of the hands and soles of the feet, producing thickened, hyperkeratotic plaques that may crack and become painful, often interfering with routine daily activities [19].
Diagnosis
The diagnosis of psoriasis is primarily clinical and is based on a detailed medical history and comprehensive dermatological examination. Characteristic erythematous plaques with silvery scales are usually sufficient for diagnosis in typical cases. When clinical findings are atypical or overlap with other dermatological conditions, a skin biopsy may be performed to confirm the diagnosis through histopathological examination. Laboratory investigations are generally not required for diagnosing psoriasis but may be useful in excluding differential diagnoses or identifying associated comorbidities. Assessment of disease severity is commonly performed using validated clinical scoring systems such as the Psoriasis Area and Severity Index (PASI), Body Surface Area (BSA), and the Dermatology Life Quality Index (DLQI), which aid in treatment planning and monitoring therapeutic response [20].
Treatment:
Apart of the treatment, we add moisturizers to get better results.
Treatment of Psoriasis
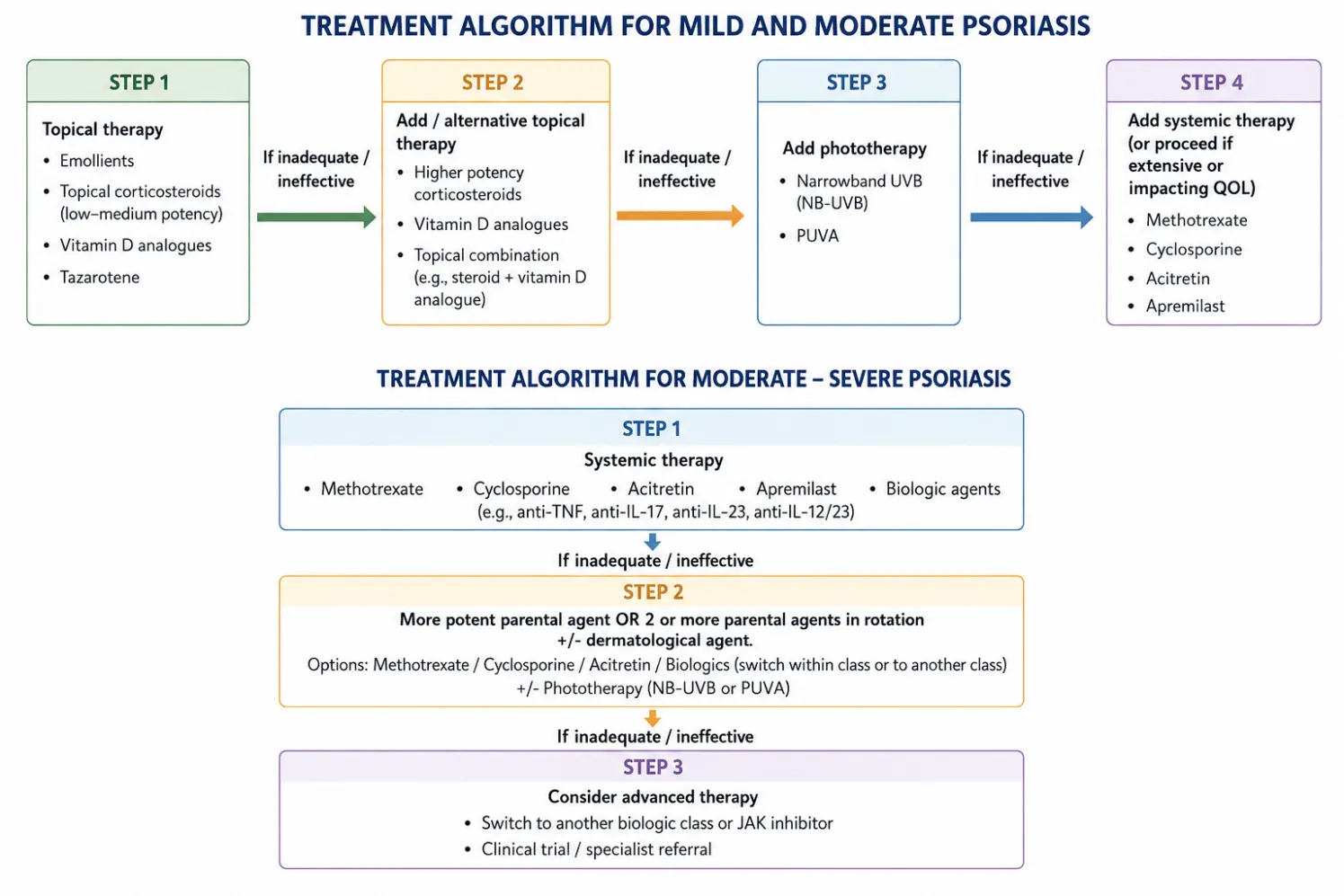
Topical Therapy
Topical medications remain the first-line treatment for patients with mild to moderate psoriasis and are aimed at reducing inflammation, controlling excessive epidermal proliferation, and relieving symptoms. Frequently prescribed topical agents include corticosteroids, coal tar preparations, anthralin, vitamin D₃ analogues such as calcipotriol, topical retinoids including tazarotene, and topical calcineurin inhibitors such as tacrolimus and pimecrolimus. The selection of topical therapy depends on disease severity, lesion location, patient preference, and treatment response [21].
Systemic Therapy
Systemic treatment is recommended for patients with moderate-to-severe psoriasis, extensive skin involvement, or inadequate response to topical therapy. Conventional oral medications include methotrexate, cyclosporine, acitretin, hydroxyurea, sulfasalazine, azathioprine, tacrolimus, and mycophenolate mofetil. In recent years, biologic agents administered by parenteral routes have become an important therapeutic option. These include alefacept, efalizumab, etanercept, infliximab, and other biologic response modifiers that selectively target immune pathways involved in the pathogenesis of psoriasis [22].
Materials and Methods
Study Design
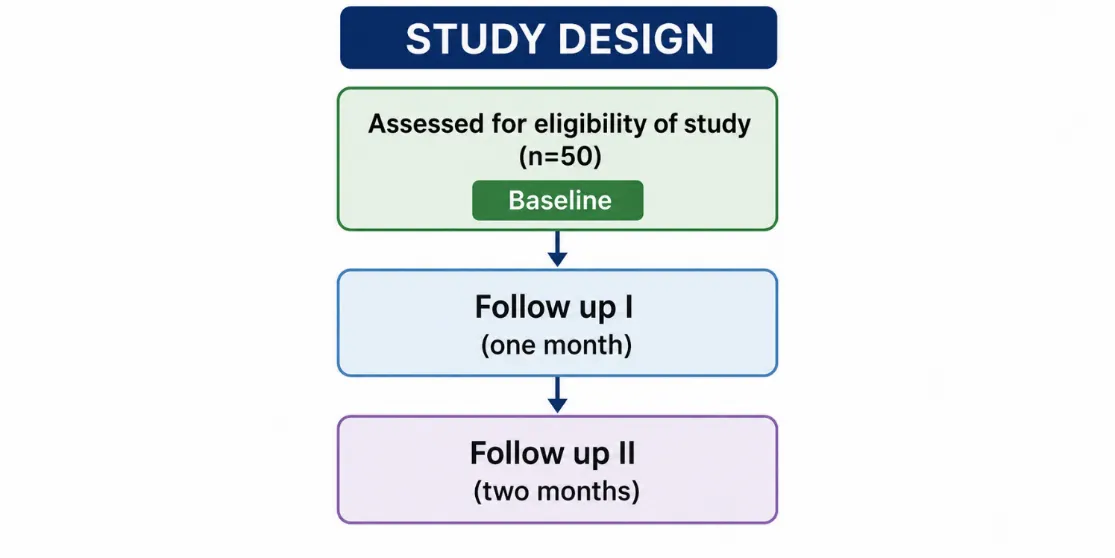
A hospital-based cross-sectional observational study was conducted among patients diagnosed with psoriasis. Eligible participants were enrolled after confirming that they fulfilled the predefined inclusion and exclusion criteria. Before participation, informed consent was obtained from all eligible patients. A structured patient data collection form was specifically developed for the study to ensure uniform documentation. The form included demographic characteristics, presenting complaints, medical and medication history, family history, personal habits, history of allergies, laboratory investigations, diagnosis, prescribed treatment, follow-up details, Psoriasis Area and Severity Index (PASI) scores, and Medication Adherence Rating Scale (MARS) scores.
Study Procedure
Baseline clinical assessment was performed at the time of enrolment. After initiation of treatment, patients were instructed to return for evaluation after one month. During the follow-up visit, participants underwent clinical examination, assessment of treatment response, and documentation of any adverse events experienced during therapy.
Disease severity was evaluated before treatment initiation and again during follow-up using the Psoriasis Area and Severity Index (PASI) [23]. Medication adherence was assessed at both visits using the Medication Adherence Rating Scale (MARS) questionnaire [24]. Changes in PASI and MARS scores between baseline and follow-up were used to evaluate clinical improvement and adherence to prescribed therapy.
Medication Adherence Assessment
Medication adherence was measured using the ten-item Medication Adherence Rating Scale (MARS). The questionnaire evaluates patients' medication-taking behaviour and identifies patterns associated with non-adherence. For items 1–6 and 9–10, a response of "No" indicated adherence and was assigned a score of 1, whereas for items 7 and 8, a response of "Yes" represented adherence and received a score of 1. The individual item scores were summed to obtain the total adherence score, with higher scores reflecting better medication adherence. The original English version of the questionnaire was used during the study. To ensure accurate understanding, each question was explained to participants in their preferred language (Telugu or Hindi), and responses were recorded accordingly.
Assessment of Disease Severity
The Psoriasis Area and Severity Index (PASI) was used to quantify disease severity [25]. This validated scoring system evaluates both the extent of body surface involvement and the severity of erythema, induration, and scaling.
The body was divided into four anatomical regions:
The final PASI score ranges from 0 to 72, with higher values indicating greater disease severity. Disease severity was classified as follows:
Sample Size
A total of 50 patients diagnosed with psoriasis were included in the study. Participant selection was carried out by the consulting dermatologist according to the predefined eligibility criteria.
Eligibility Criteria
Inclusion Criteria
Exclusion Criteria
Study Materials
The following tools and resources were used during the study:
Study Workflow
The study was conducted according to the following sequence:
Data Analysis
The collected data were entered into Microsoft Excel and analyzed using descriptive statistical methods. Continuous variables were summarized as mean ± standard deviation (SD), whereas categorical variables were presented as frequencies and percentages. Baseline demographic characteristics, prevalence of psoriasis, disease severity assessed using the Psoriasis Area and Severity Index (PASI), medication adherence evaluated using the Medication Adherence Rating Scale (MARS), treatment patterns, and associated clinical characteristics were analyzed descriptively.
RESULTS
Prevalence of Psoriasis
During the six-month study period, a total of 8,720 patients attended the dermatology outpatient department. Among them, 50 patients were diagnosed with psoriasis, resulting in a hospital-based prevalence of 0.57%.
|
Total dermatology patients |
Patients diagnosed with psoriasis |
Prevalence |
|
8720 |
50 |
0.57% |
Age Distribution
The study included 50 male patients diagnosed with psoriasis. The largest proportion of patients belonged to the 46–60 years age group (40%), followed by the 31–45 years and >61 years groups, each accounting for 22%. Patients aged 16–30 years represented 16% of the study population.
|
Age group (years) |
Number |
Percentage |
|
16–30 |
8 |
16% |
|
31–45 |
11 |
22% |
|
46–60 |
20 |
40% |
|
>61 |
11 |
22% |
The findings indicate that psoriasis was most frequently observed among middle-aged adults.
Associated Comorbidities
Hypertension was the most commonly reported coexisting medical condition, affecting 22% of patients. Diabetes mellitus was present in 6% of participants, while the remaining 72% had no documented comorbid illness.
|
Comorbidity |
Number |
Percentage |
|
Hypertension |
11 |
22% |
|
Diabetes mellitus |
3 |
6% |
|
None |
36 |
72% |
Employment Status
Among the study participants, 28 patients (56%) were employed, whereas 22 patients (44%) were unemployed.
|
Employment status |
Number |
Percentage |
|
Employed |
28 |
56% |
|
Unemployed |
22 |
44% |
Personal Habits
Most participants (72%) reported no history of smoking or alcohol consumption. Smoking alone was reported by 8%, alcohol consumption alone by 10%, and both smoking and alcohol use by 10% of patients.
|
Personal habit |
Number |
Percentage |
|
Smoking |
4 |
8% |
|
Alcohol consumption |
5 |
10% |
|
Smoking and alcohol |
5 |
10% |
|
None |
36 |
72% |
Clinical Types of Psoriasis
The most frequently documented clinical presentations were chronic plaque psoriasis and psoriasis vulgaris, each accounting for 36% of cases. Palmoplantar psoriasis constituted 14%, while the remaining clinical variants were observed less frequently.
|
Clinical type |
Number |
Percentage |
|
Chronic plaque psoriasis |
18 |
36% |
|
Psoriasis vulgaris |
18 |
36% |
|
Palmoplantar psoriasis |
7 |
14% |
|
Sebopsoriasis |
2 |
4% |
|
Guttate psoriasis |
1 |
2% |
|
Nail psoriasis |
1 |
2% |
|
Scalp psoriasis |
1 |
2% |
|
Erythrodermic psoriasis |
1 |
2% |
|
Generalized plaque psoriasis |
1 |
2% |
Changes in Disease Severity
Disease severity was evaluated using PASI scores at baseline and after one month of treatment. At baseline, mild, moderate, and severe psoriasis were observed in 34%, 34%, and 32% of patients, respectively. At the first follow-up, the proportion of patients with mild disease increased to 52%, while severe disease decreased to 12%, suggesting an overall improvement in clinical status following treatment.
|
Disease severity |
Baseline |
First follow-up |
|
Mild (PASI <5) |
17 |
26 |
|
Moderate (PASI 5–10) |
17 |
18 |
|
Severe (PASI >10) |
16 |
6 |
The mean PASI score declined from 8.27 ± 5.70 at baseline to 5.43 ± 3.69 during follow-up, demonstrating a reduction in disease severity.
|
Assessment |
Mean ± SD |
|
Baseline PASI |
8.27 ± 5.70 |
|
First follow-up PASI |
5.43 ± 3.69 |
Treatment Profile
Patients received a combination of topical and systemic therapies according to disease severity and clinical requirements. Cetirizine was the most frequently prescribed medication (94%), followed by Vitamin A & D preparations (78%), betamethasone cream (64%), calcium supplements (60%), Vitamin B-complex (48%), and LPF lotion (42%). Methotrexate was prescribed to 20% of patients with more extensive disease.
|
Medication |
Number |
Percentage |
|
Cetirizine |
47 |
94% |
|
Vitamin A & D |
39 |
78% |
|
Betamethasone cream |
32 |
64% |
|
Calcium |
30 |
60% |
|
Vitamin B-complex |
24 |
48% |
|
LPF lotion |
21 |
42% |
|
Methotrexate |
10 |
20% |
|
Moyzen oil |
10 |
20% |
|
Vitamin D₃ |
8 |
16% |
|
Cefixime |
6 |
12% |
|
Pantoprazole |
6 |
12% |
|
Amoxiclav |
5 |
10% |
|
Folic acid |
3 |
6% |
Medication Adherence
Medication adherence improved following pharmacist-led counselling and follow-up. The mean MARS score increased from 4.74 ± 0.72 at baseline to 7.08 ± 1.31 after one month of treatment, indicating better adherence to prescribed medications.
|
Assessment |
Mean ± SD |
|
Baseline MARS |
4.74 ± 0.72 |
|
First follow-up MARS |
7.08 ± 1.31 |
CONCLUSION
The present study demonstrated that structured clinical pharmacist involvement was associated with improved medication adherence and better clinical outcomes among patients with psoriasis. A significant reduction in PASI scores together with improved MARS scores suggests that patient education, regular counselling, and systematic follow-up can positively influence treatment adherence and disease control. Given the chronic and relapsing nature of psoriasis, effective management requires continuous collaboration between dermatologists, clinical pharmacists, nurses, and patients. Clinical pharmacists can contribute by providing medication counselling, identifying drug-related problems, reinforcing adherence, monitoring adverse effects, and supporting individualized treatment plans. Future investigations involving larger and more diverse patient populations with longer follow-up periods are warranted to evaluate the long-term impact of pharmacist-led interventions on disease control, quality of life, treatment persistence, and healthcare utilization. Such studies may also explore the influence of socioeconomic, psychological, and behavioural factors on adherence to optimize comprehensive psoriasis management.
REFERENCES

Mohana Priya Pamidi*, K. Venkata Gopaiah, Medication Adherence to Treatment Among Patients with Psoriasis: A Hospital-Based Observational Study, Int. J. Med. Pharm. Sci., 2026, 2 (7), 703-712. https://doi.org/10.5281/zenodo.21376950
 10.5281/zenodo.21376950
10.5281/zenodo.21376950