
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1Department of Pharmaceutical Sciences, Gurukul Kangri (Deemed to be University), Haridwar, Uttarakhand, India.
2Department of Pharmacy, Bhagwant Global University, Kotdwar, Uttarakhand, India.
3Shri Ram College of Pharmacy, Muzaffarnagar, Uttar Pradesh, India.
4Department of Pharmacy, Glocal University, Saharanpur, Uttar Pradesh, India
Quetiapine is a second-generation antipsychotic widely prescribed for schizophrenia and bipolar disorder and is increasingly encountered in clinical practice for its sedative properties. Although improvement in sleep is frequently observed during quetiapine therapy, the neuropharmacological mechanisms responsible for its sleep-promoting effects remain a topic of ongoing investigation. This review critically examines the current understanding of quetiapine-induced sleep by integrating evidence from receptor pharmacology, sleep physiology, pharmacokinetics, and clinical studies. The sedative effects of quetiapine are primarily attributed to potent antagonism of histamine H1 receptors, accompanied by blockade of serotonin 5-HT2A and α1-adrenergic receptors, while comparatively lower dopamine D2 receptor occupancy at low doses contributes to reduced extrapyramidal adverse effects. These receptor interactions facilitate sleep initiation, decrease sleep latency, and may improve subjective sleep quality in selected patient populations. The review further discusses dose-dependent differences in sedation, the contribution of the active metabolite norquetiapine, and the influence of quetiapine on sleep architecture. Available clinical evidence supporting its use in schizophrenia and bipolar disorder is evaluated alongside the more controversial off-label use for primary insomnia, where the balance between potential benefit and long-term safety remains uncertain. Particular attention is given to adverse effects, including daytime somnolence, metabolic disturbances, orthostatic hypotension, and the need for careful patient selection. By synthesizing current pharmacological and clinical evidence, this review provides a balanced perspective on the mechanisms underlying quetiapine-associated sleep promotion and highlights important considerations for rational and evidence-based clinical practice.
Sleep is a fundamental biological process that plays a central role in maintaining cognitive performance, emotional regulation, metabolic homeostasis, immune competence, and overall health. Disruption of normal sleep is common among individuals with psychiatric disorders, particularly schizophrenia and bipolar disorder, where insomnia, fragmented sleep, prolonged sleep latency, and alterations in sleep architecture frequently accompany the primary illness. Persistent sleep disturbances not only impair quality of life but are also associated with symptom exacerbation, reduced treatment adherence, cognitive dysfunction, and an increased risk of relapse. Consequently, restoration of healthy sleep has become an important therapeutic objective in modern psychiatric care. Quetiapine is a second-generation (atypical) antipsychotic approved for the treatment of schizophrenia, bipolar disorder, and, in some regions, as an adjunctive therapy for major depressive disorder. Beyond its established antipsychotic efficacy, quetiapine has attracted considerable clinical attention because of its pronounced sedative effects, particularly at relatively low doses. Many patients receiving quetiapine report earlier sleep onset, reduced nocturnal awakenings, and improved subjective sleep quality. These observations have contributed to its widespread off-label use for insomnia despite continuing debate regarding its long-term safety and the strength of supporting clinical evidence. Unlike conventional hypnotic agents that primarily enhance γ-aminobutyric acid (GABA)-mediated neurotransmission, quetiapine promotes sleep through a complex interaction with multiple neurotransmitter systems. Its high affinity for histamine H1 receptors, together with antagonism of serotonin 5-hydroxytryptamine-2A (5-HT2A) and α1-adrenergic receptors, is considered the principal pharmacological basis for its sleep-promoting properties. In contrast, dopamine D2 receptor occupancy is comparatively lower at doses commonly associated with sedation, allowing significant hypnotic effects without producing the degree of motor adverse effects typically observed with many first-generation antipsychotics. Furthermore, the active metabolite norquetiapine possesses distinct pharmacological characteristics that may further influence sleep regulation and overall therapeutic response. Although the sedative properties of quetiapine are well recognized in clinical practice, important questions remain regarding the precise mechanisms underlying its effects on sleep architecture, the relationship between receptor occupancy and dose-dependent sedation, and the balance between therapeutic benefit and potential adverse outcomes. Long-term administration may be associated with metabolic abnormalities, excessive daytime somnolence, orthostatic hypotension, and other clinically relevant safety concerns that necessitate careful patient selection and individualized risk-benefit assessment. Over the past decade, advances in neuropharmacology and sleep medicine have substantially improved understanding of the biological pathways involved in quetiapine-induced sleep. Nevertheless, available evidence remains dispersed across experimental studies, clinical trials, observational research, and narrative reviews, making comprehensive interpretation challenging for clinicians and researchers. An integrated evaluation of these findings is therefore necessary to clarify the current state of knowledge and identify areas requiring further investigation. The objective of the present review is to critically examine the neuropharmacological mechanisms responsible for quetiapine-induced sleep, evaluate its effects on sleep physiology and sleep architecture, summarize available clinical evidence across psychiatric disorders and off-label insomnia, discuss dose-dependent pharmacological characteristics, and highlight important safety considerations and future research priorities. By synthesizing current evidence, this review aims to provide a scientifically balanced and clinically relevant understanding of how quetiapine promotes sleep and its appropriate role in contemporary pharmacotherapy.
Table 1. Major Neurotransmitter Receptors Involved in Sleep Regulation and Their Pharmacological Modulation by Quetiapine
|
Neurotransmitter System |
Primary Physiological Role in Sleep |
Action of Quetiapine |
Expected Clinical Effect |
|
Histamine (H1) |
Maintains wakefulness |
Strong H1 receptor antagonism |
Sedation and facilitation of sleep onset |
|
Serotonin (5-HT2A) |
Modulates sleep continuity and slow-wave sleep |
Receptor antagonism |
Improved sleep continuity and reduced sleep latency |
|
Adrenergic (α1) |
Promotes arousal |
Receptor antagonism |
Reduced central arousal and enhanced sleep initiation |
|
Dopamine (D2) |
Regulates motivation and wakefulness |
Moderate antagonism (dose dependent) |
Antipsychotic effect with relatively lower extrapyramidal symptoms at low doses |
|
Muscarinic (M1) |
Cognitive function and REM regulation |
Mild antagonism |
Limited contribution to sedation with potential anticholinergic effects |
2. Sleep Physiology
Sleep is a highly organized and dynamic neurobiological process regulated by complex interactions among neuronal networks, neurotransmitters, circadian rhythms, and homeostatic mechanisms. Rather than representing a passive state of unconsciousness, sleep is an active physiological process that is essential for brain function, metabolic regulation, immune competence, emotional stability, learning, and memory consolidation. The timing, duration, and quality of sleep are primarily governed by two complementary regulatory systems: the circadian timing system and the homeostatic sleep drive. The circadian rhythm is controlled by the suprachiasmatic nucleus (SCN) of the anterior hypothalamus, which functions as the body's central biological clock. Environmental light signals received through the retina synchronize the SCN with the external light-dark cycle, thereby regulating the secretion of melatonin from the pineal gland and coordinating the sleep–wake cycle. In parallel, the homeostatic sleep process increases the physiological drive for sleep during prolonged wakefulness and gradually dissipates as restorative sleep occurs. The interaction between these two regulatory mechanisms determines the initiation, maintenance, and termination of normal sleep. Normal human sleep consists of two major physiological states: non-rapid eye movement (NREM) sleep and rapid eye movement (REM) sleep. These stages alternate cyclically throughout the night, with each sleep cycle typically lasting approximately 90–110 minutes in healthy adults. NREM sleep accounts for the majority of total sleep time and is subdivided into three stages (N1, N2, and N3), each characterized by distinct electrophysiological and physiological features. Stage N1 represents the transition from wakefulness to sleep and is associated with reduced muscle activity and slowing of eye movements. Stage N2 is characterized by sleep spindles and K-complexes on electroencephalography (EEG), reflecting reduced responsiveness to external stimuli and stabilization of sleep. Stage N3, commonly referred to as slow-wave sleep or deep sleep, exhibits high-amplitude, low-frequency delta waves and plays a critical role in physical restoration, immune regulation, growth hormone secretion, and memory consolidation. REM sleep differs markedly from NREM sleep in both neurophysiology and function. It is characterized by rapid eye movements, skeletal muscle atonia, cortical activation, vivid dreaming, and increased autonomic variability. REM sleep contributes significantly to emotional processing, procedural learning, and cognitive integration. Under normal physiological conditions, REM periods become progressively longer during the latter half of the night, whereas slow-wave sleep predominates during the initial sleep cycles. The transition between wakefulness and sleep is regulated by coordinated changes in multiple neurotransmitter systems. Histaminergic neurons originating from the tuberomammillary nucleus promote wakefulness through activation of histamine H1 receptors. Similarly, noradrenergic neurons of the locus coeruleus, serotonergic neurons of the dorsal raphe nucleus, cholinergic neurons of the basal forebrain and pontine tegmentum, and dopaminergic pathways collectively contribute to maintaining cortical arousal. Sleep initiation occurs when the activity of these wake-promoting systems is suppressed while sleep-promoting neurons located within the ventrolateral preoptic nucleus (VLPO) release γ-aminobutyric acid (GABA) and galanin, thereby inhibiting arousal networks. Among these neurotransmitter systems, histamine has a particularly important role in sustaining wakefulness. Pharmacological inhibition of histamine H1 receptors consistently produces sedation and facilitates sleep initiation, explaining why medications possessing strong H1 receptor antagonism frequently induce drowsiness. Serotonergic and adrenergic pathways also participate in regulating sleep continuity and arousal, while dopaminergic neurotransmission influences motivation, alertness, and behavioral activation. The coordinated modulation of these pathways forms the neurobiological foundation for the sleep-promoting effects observed with several psychotropic medications, including quetiapine. Understanding normal sleep physiology provides an essential framework for interpreting the pharmacological actions of quetiapine. Its sedative effects cannot be attributed to a single receptor or neurotransmitter but instead arise from simultaneous modulation of multiple wake-promoting pathways. Consequently, an appreciation of normal sleep regulation is fundamental for understanding the receptor-mediated mechanisms through which quetiapine facilitates sleep initiation, improves sleep continuity, and alters overall sleep architecture.
Table 2. Physiological Characteristics of Normal Sleep Stages
|
Sleep Stage |
Major Physiological Characteristics |
Primary Physiological Functions |
|
N1 (Stage 1) |
Transition from wakefulness; slow eye movements; reduced muscle activity |
Sleep initiation and transition to stable sleep |
|
N2 (Stage 2) |
Presence of sleep spindles and K-complexes; reduced responsiveness to external stimuli |
Sleep maintenance, sensory processing, and memory consolidation |
|
N3 (Slow-Wave Sleep) |
High-amplitude delta waves; deepest stage of NREM sleep |
Physical restoration, immune function, growth hormone secretion, and memory consolidation |
|
REM Sleep |
Rapid eye movements, vivid dreaming, skeletal muscle atonia, cortical activation |
Emotional regulation, procedural learning, memory integration, and cognitive processing |
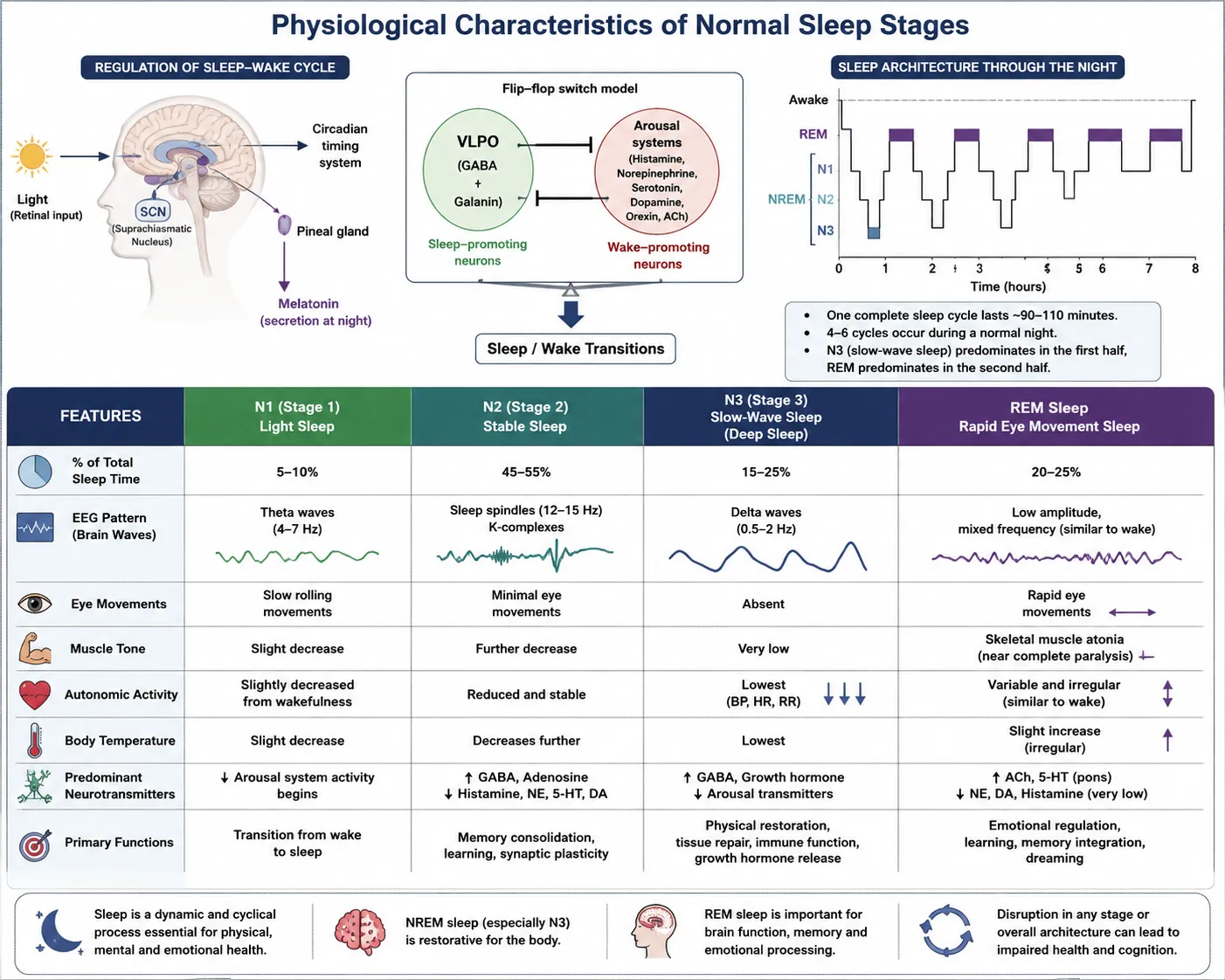
Figure 1. Physiological Characteristics of Normal Sleep Stages
2.1 Physiological Regulation of the Sleep–Wake Cycle
The sleep–wake cycle is a highly coordinated physiological process that maintains the balance between periods of wakefulness and sleep through the integrated activity of multiple neural circuits, neurotransmitter systems, and regulatory mechanisms. Rather than functioning as an "on–off" phenomenon, sleep and wakefulness represent dynamic physiological states that continuously interact to preserve optimal brain function, behavioral performance, and systemic homeostasis. The transition between these states is regulated by reciprocal interactions between sleep-promoting and wake-promoting neuronal networks located within the hypothalamus, brainstem, basal forebrain, and cerebral cortex. Wakefulness is maintained by the ascending arousal system, a distributed neuronal network that projects from the brainstem and hypothalamus to widespread cortical and subcortical regions. This system comprises several neurotransmitter-specific nuclei, including histaminergic neurons of the tuberomammillary nucleus, noradrenergic neurons of the locus coeruleus, serotonergic neurons of the dorsal raphe nucleus, cholinergic neurons of the pedunculopontine and laterodorsal tegmental nuclei, dopaminergic neurons of the ventral tegmental area, and orexin-producing neurons of the lateral hypothalamus. The coordinated activation of these pathways sustains cortical arousal, attention, cognitive performance, and behavioral responsiveness during wakefulness. In contrast, sleep initiation is primarily mediated by neurons located within the ventrolateral preoptic nucleus (VLPO) of the anterior hypothalamus. These neurons release γ-aminobutyric acid (GABA) and galanin, inhibitory neurotransmitters that suppress the activity of wake-promoting nuclei. Progressive inhibition of the ascending arousal system reduces cortical activation and facilitates the transition from wakefulness to non-rapid eye movement (NREM) sleep. The reciprocal inhibitory relationship between VLPO neurons and arousal-promoting pathways is commonly described as a "flip-flop switch", a mechanism that enables rapid and stable transitions between sleep and wake states while minimizing intermediate states of consciousness. The orexin (hypocretin) system provides additional stabilization of the sleep–wake cycle by reinforcing wake-promoting neuronal activity and preventing inappropriate transitions into sleep. Orexinergic neurons located in the lateral hypothalamus project extensively throughout the central nervous system and stimulate multiple arousal centers. Loss of orexin signaling has been strongly associated with unstable sleep–wake regulation and disorders such as narcolepsy, highlighting its essential role in maintaining sustained wakefulness. The physiological regulation of sleep also depends upon close interaction between neuronal activity and circadian timing mechanisms. As wakefulness is prolonged, homeostatic sleep pressure gradually increases owing to the accumulation of sleep-promoting metabolites, including adenosine, within the brain. Simultaneously, the circadian pacemaker located in the suprachiasmatic nucleus coordinates daily fluctuations in alertness, hormonal secretion, body temperature, and other biological rhythms. Together, these homeostatic and circadian processes determine the timing, duration, and quality of sleep. Multiple neurotransmitters contribute to the regulation of the sleep–wake cycle through complementary physiological functions. Histamine promotes cortical activation and wakefulness through histamine H1 receptors, whereas norepinephrine and serotonin maintain vigilance and behavioral alertness. Dopamine influences motivation, reward processing, and arousal, while acetylcholine facilitates cortical activation during both wakefulness and rapid eye movement (REM) sleep. Conversely, GABA serves as the principal inhibitory neurotransmitter responsible for suppressing arousal networks and promoting sleep onset. The coordinated balance among these neurotransmitter systems ensures normal cycling between wakefulness, NREM sleep, and REM sleep. Understanding the physiological regulation of the sleep–wake cycle is fundamental for interpreting the pharmacological actions of quetiapine. Unlike conventional hypnotic agents that primarily potentiate GABAergic neurotransmission, quetiapine promotes sleep predominantly through antagonism of several wake-promoting neurotransmitter receptors, particularly histamine H1, serotonin 5-HT2A, and α1-adrenergic receptors. Consequently, a clear understanding of normal sleep–wake regulation provides the neurobiological foundation for explaining the sedative properties and clinical sleep-promoting effects of quetiapine discussed in subsequent sections of this review.
Table 3. Major Neural Structures and Neurotransmitter Systems Involved in the Physiological Regulation of the Sleep–Wake Cycle
|
Neural Structure / Brain Region |
Principal Neurotransmitter(s) |
Primary Physiological Function |
Role in Sleep–Wake Regulation |
|
Suprachiasmatic Nucleus (SCN) |
GABA, vasoactive intestinal peptide (VIP), arginine vasopressin (AVP) |
Central circadian pacemaker |
Synchronizes the sleep–wake cycle with the environmental light–dark cycle and regulates circadian rhythms. |
|
Ventrolateral Preoptic Nucleus (VLPO) |
GABA, Galanin |
Sleep-promoting center |
Inhibits wake-promoting nuclei, facilitating sleep initiation and maintenance, particularly during NREM sleep. |
|
Lateral Hypothalamus |
Orexin (Hypocretin) |
Stabilization of wakefulness |
Activates arousal systems and prevents inappropriate transitions from wakefulness to sleep. |
|
Tuberomammillary Nucleus (TMN) |
Histamine |
Promotion of cortical arousal |
Maintains wakefulness through activation of histamine H1 receptors; reduced activity facilitates sleep onset. |
|
Locus Coeruleus (LC) |
Norepinephrine |
Attention and vigilance |
High activity during wakefulness, decreases during NREM sleep, and is nearly silent during REM sleep. |
|
Dorsal Raphe Nucleus (DRN) |
Serotonin (5-HT) |
Modulation of arousal and mood |
Contributes to wakefulness and influences sleep continuity and sleep-stage transitions. |
|
Pedunculopontine and Laterodorsal Tegmental Nuclei (PPT/LDT) |
Acetylcholine |
Cortical activation |
Active during wakefulness and REM sleep; contributes to REM generation and cortical activation. |
|
Ventral Tegmental Area (VTA) |
Dopamine |
Motivation, reward, and arousal |
Participates in behavioral arousal and modulation of wakefulness. |
|
Basal Forebrain |
Acetylcholine, GABA |
Cortical activation and cognitive processing |
Supports wakefulness and attention while participating in transitions between sleep stages. |
2.2 Circadian Rhythm and Homeostatic Control of Sleep
Normal sleep is regulated by the coordinated interaction of two fundamental biological processes: the circadian timing system and the homeostatic sleep drive. These complementary mechanisms determine the timing, duration, and quality of sleep while ensuring appropriate alignment of physiological functions with environmental and behavioral demands. The integration of these regulatory systems enables individuals to maintain stable sleep–wake patterns under normal physiological conditions and adapt to daily fluctuations in activity and environmental light exposure. The circadian rhythm is an endogenous biological rhythm with an approximately 24-hour periodicity that governs numerous physiological processes, including the sleep–wake cycle, hormone secretion, body temperature, metabolism, and cognitive performance. The master circadian pacemaker is located within the suprachiasmatic nucleus (SCN) of the anterior hypothalamus. Specialized intrinsically photosensitive retinal ganglion cells detect environmental light and transmit photic information to the SCN through the retinohypothalamic tract. This light-dependent signaling synchronizes the internal biological clock with the external light–dark cycle, thereby maintaining circadian alignment. The SCN coordinates circadian rhythms by regulating neural and endocrine pathways that influence sleep propensity and wakefulness. One of its most important downstream effects is the modulation of melatonin secretion by the pineal gland. As ambient light decreases during the evening, reduced photic stimulation of the SCN permits melatonin release, promoting physiological readiness for sleep. Conversely, exposure to daylight suppresses melatonin secretion and facilitates wakefulness. In addition to regulating melatonin, the SCN influences daily fluctuations in core body temperature, cortisol secretion, autonomic nervous system activity, and behavioral alertness, all of which contribute to the temporal organization of sleep. Complementing circadian regulation, the homeostatic sleep process reflects the progressive accumulation of sleep pressure during wakefulness. The longer an individual remains awake, the greater the physiological drive to initiate sleep. This homeostatic pressure is believed to be mediated, in part, by the accumulation of adenosine within the basal forebrain and other brain regions. Adenosine acts as an inhibitory neuromodulator that suppresses wake-promoting neuronal activity while enhancing the activity of sleep-promoting neurons within the ventrolateral preoptic nucleus (VLPO). During sleep, adenosine concentrations gradually decline, resulting in the dissipation of sleep pressure and restoration of normal alertness upon awakening. The interaction between circadian timing and homeostatic sleep pressure is commonly described by the two-process model of sleep regulation. According to this model, Process C (Circadian Process) regulates the timing of sleep and wakefulness based on endogenous biological rhythms, whereas Process S (Homeostatic Process) reflects the increasing physiological need for sleep as wakefulness is prolonged. Sleep is initiated when homeostatic sleep pressure becomes sufficiently strong while the circadian system simultaneously promotes sleep. Conversely, awakening occurs as homeostatic pressure decreases and circadian mechanisms promote arousal. The continuous interaction between these two processes ensures the consolidation of nocturnal sleep and the maintenance of daytime wakefulness. Disruption of either circadian or homeostatic regulation may lead to significant alterations in sleep quality and duration. Circadian misalignment resulting from shift work, transmeridian travel, irregular sleep schedules, or excessive exposure to artificial light during the evening can delay sleep onset and reduce sleep efficiency. Similarly, disturbances in homeostatic sleep regulation may contribute to insomnia, excessive daytime sleepiness, and fragmented sleep. These disturbances are particularly common in individuals with psychiatric disorders, where abnormalities in circadian rhythms and neurotransmitter function frequently coexist. Understanding the physiological interaction between circadian and homeostatic mechanisms is essential for interpreting the sleep-promoting effects of quetiapine. Although quetiapine is not a primary circadian regulator, its antagonistic actions on wake-promoting neurotransmitter systems reduce physiological arousal and facilitate sleep initiation when endogenous sleep pressure is present. Consequently, its clinical effects on sleep should be interpreted within the broader context of normal circadian biology and homeostatic sleep regulation.
Table 4. Comparison of Circadian and Homeostatic Mechanisms Regulating Human Sleep
|
Characteristic |
Circadian Process (Process C) |
Homeostatic Process (Process S) |
|
Primary regulator |
Suprachiasmatic nucleus (SCN) |
Accumulated sleep pressure during wakefulness |
|
Main physiological role |
Determines the timing of sleep and wakefulness |
Determines the physiological need for sleep |
|
Major biological signal |
Environmental light–dark cycle |
Duration of prior wakefulness |
|
Important mediator |
Melatonin secretion |
Adenosine accumulation |
|
Activity during prolonged wakefulness |
Continues rhythmic oscillation |
Progressively increases |
|
Activity during sleep |
Maintains circadian timing |
Gradually dissipates |
|
Principal outcome |
Synchronization of biological rhythms |
Initiation and maintenance of restorative sleep |
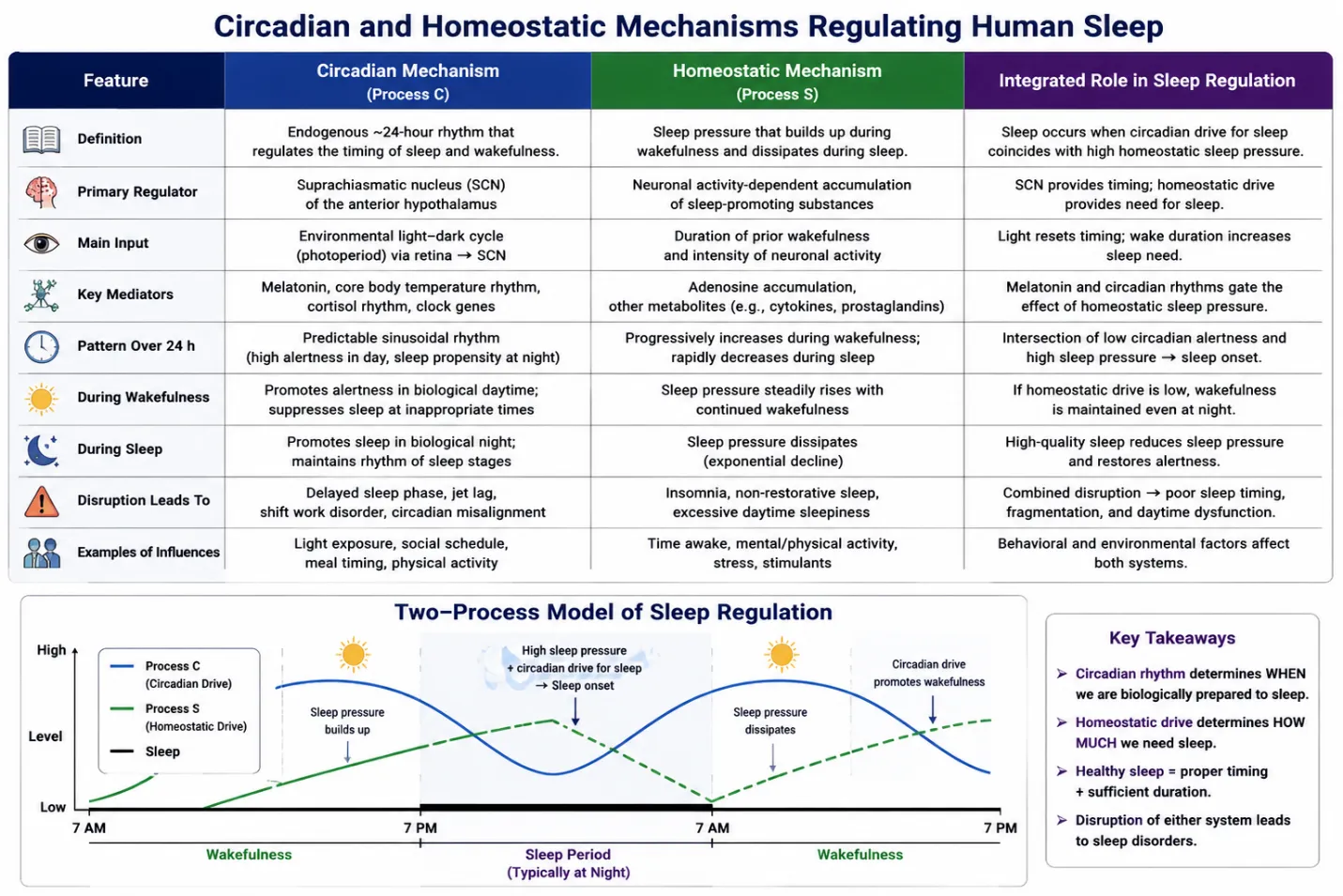
Figure 2. Circadian and Homeostatic Mechanisms Regulating Human Sleep
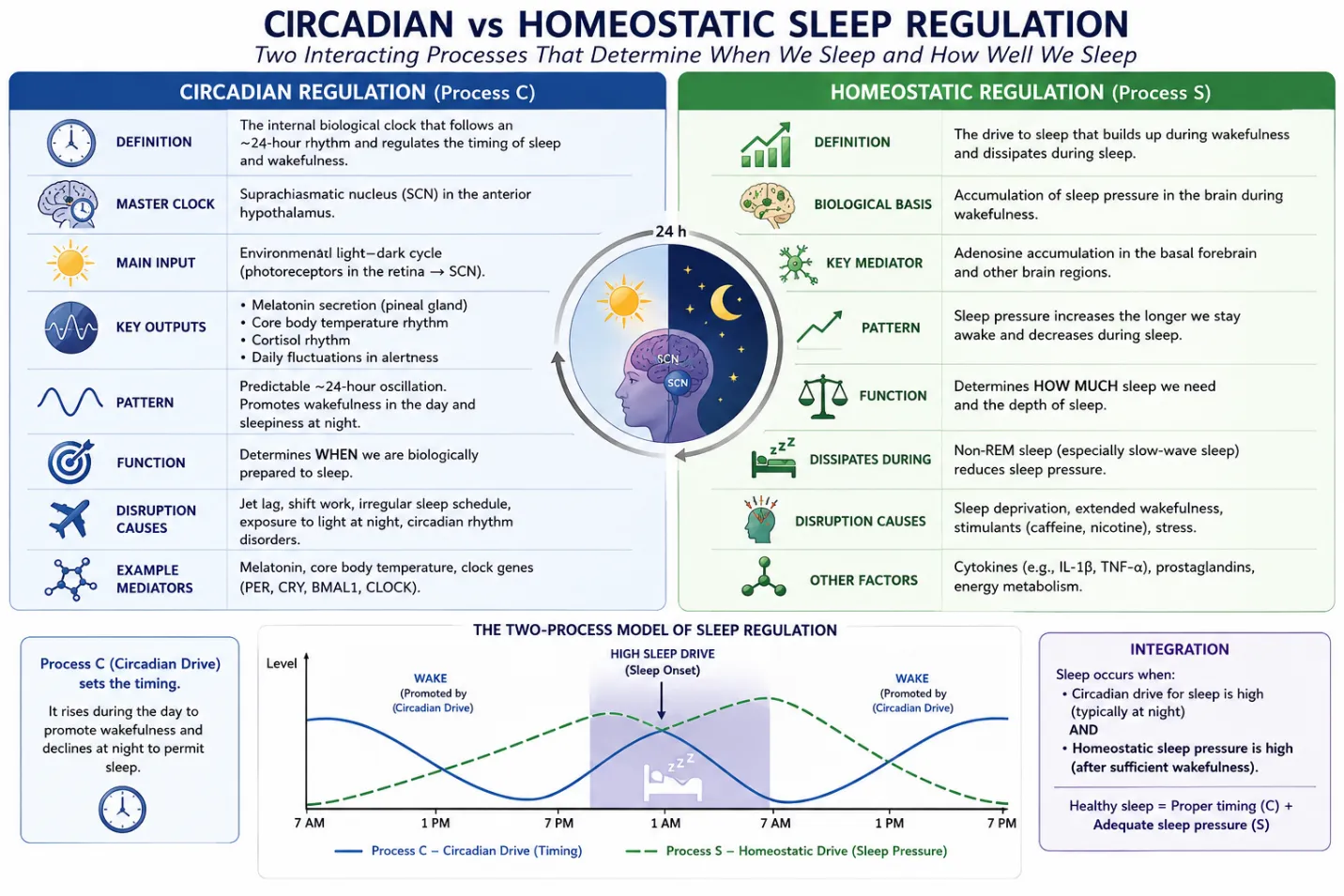
Figure 3. Circadian vs homeostatic sleep regulation
2.3 Sleep Architecture: Non-Rapid Eye Movement (NREM) and Rapid Eye Movement (REM) Sleep
Sleep architecture refers to the characteristic organization and cyclic distribution of sleep stages throughout a normal sleep period. In healthy adults, sleep is composed of two physiologically distinct states: non-rapid eye movement (NREM) sleep and rapid eye movement (REM) sleep. These stages alternate in a predictable pattern, forming repetitive sleep cycles that typically last approximately 90–110 minutes. A normal night's sleep generally consists of four to six such cycles, with the relative proportion of each stage varying across the night. Early sleep cycles are dominated by deep NREM sleep, whereas REM sleep progressively increases in duration during the latter part of the night. This dynamic organization is essential for maintaining physiological restoration, cognitive function, emotional regulation, and memory consolidation. NREM sleep constitutes approximately 75–80% of total sleep time and is subdivided into three stages designated as N1, N2, and N3 according to the American Academy of Sleep Medicine (AASM) classification. Each stage represents a progressive reduction in cortical arousal and increasing depth of sleep.
Stage N1 is the lightest stage of sleep and serves as the transition between wakefulness and stable sleep. It is characterized by reduced muscle tone, slow rolling eye movements, and low-amplitude theta-wave activity on electroencephalography (EEG). Individuals are easily aroused during this stage and may experience transient muscle contractions or the sensation of falling as consciousness gradually diminishes.
Stage N2 represents the predominant stage of normal sleep and is characterized by the appearance of sleep spindles and K-complexes on EEG recordings. Sleep spindles are brief bursts of synchronized neuronal activity that are believed to contribute to memory consolidation, synaptic plasticity, and protection against external sensory disturbances. K-complexes are large biphasic waveforms that facilitate sleep maintenance while allowing selective responsiveness to potentially significant environmental stimuli. Physiologically, body temperature, heart rate, and metabolic activity decline further during this stage, promoting stable and restorative sleep.
Stage N3, also known as slow-wave sleep (SWS) or deep sleep, represents the deepest phase of NREM sleep and is characterized by high-amplitude, low-frequency delta waves. This stage plays a fundamental role in physical restoration, tissue repair, immune regulation, and growth hormone secretion. Slow-wave sleep is also critically involved in memory consolidation, particularly declarative memory, and contributes to recovery from physical and mental fatigue. Because arousal thresholds are highest during this stage, awakening an individual from N3 sleep is often associated with transient disorientation or sleep inertia.
In contrast to NREM sleep, rapid eye movement (REM) sleep exhibits neurophysiological characteristics that closely resemble wakefulness despite profound skeletal muscle atonia. REM sleep is characterized by rapid conjugate eye movements, low-amplitude mixed-frequency EEG activity, vivid dreaming, irregular autonomic activity, and near-complete suppression of skeletal muscle tone mediated by brainstem inhibitory pathways. This physiological muscle paralysis prevents the execution of complex motor behaviors during dreaming while preserving respiratory and ocular muscle function. REM sleep plays a critical role in emotional regulation, procedural learning, memory integration, and higher cognitive processing. Cholinergic neuronal activity increases substantially during REM sleep, whereas the activity of noradrenergic and serotonergic neurons declines markedly. This unique neurochemical environment contributes to cortical activation, dream generation, and selective processing of emotional and procedural memories. As the night progresses, REM episodes become progressively longer, accounting for a greater proportion of total sleep time during the early morning hours. The normal alternation between NREM and REM sleep is regulated through coordinated interactions among circadian mechanisms, homeostatic sleep pressure, and multiple neurotransmitter systems. Disturbances in sleep architecture may adversely affect cognitive performance, mood regulation, metabolic homeostasis, and cardiovascular health. Such alterations are frequently observed in psychiatric disorders, including schizophrenia and bipolar disorder, where abnormalities in sleep continuity, slow-wave sleep, and REM organization are commonly reported. Understanding normal sleep architecture is particularly important for evaluating the pharmacological effects of quetiapine. By modulating several wake-promoting neurotransmitter systems, quetiapine has the potential to influence sleep initiation, sleep continuity, and the distribution of NREM and REM sleep. Consequently, knowledge of normal sleep architecture provides the physiological framework for interpreting the clinical evidence regarding quetiapine-associated improvements in sleep quality discussed in subsequent sections of this review.
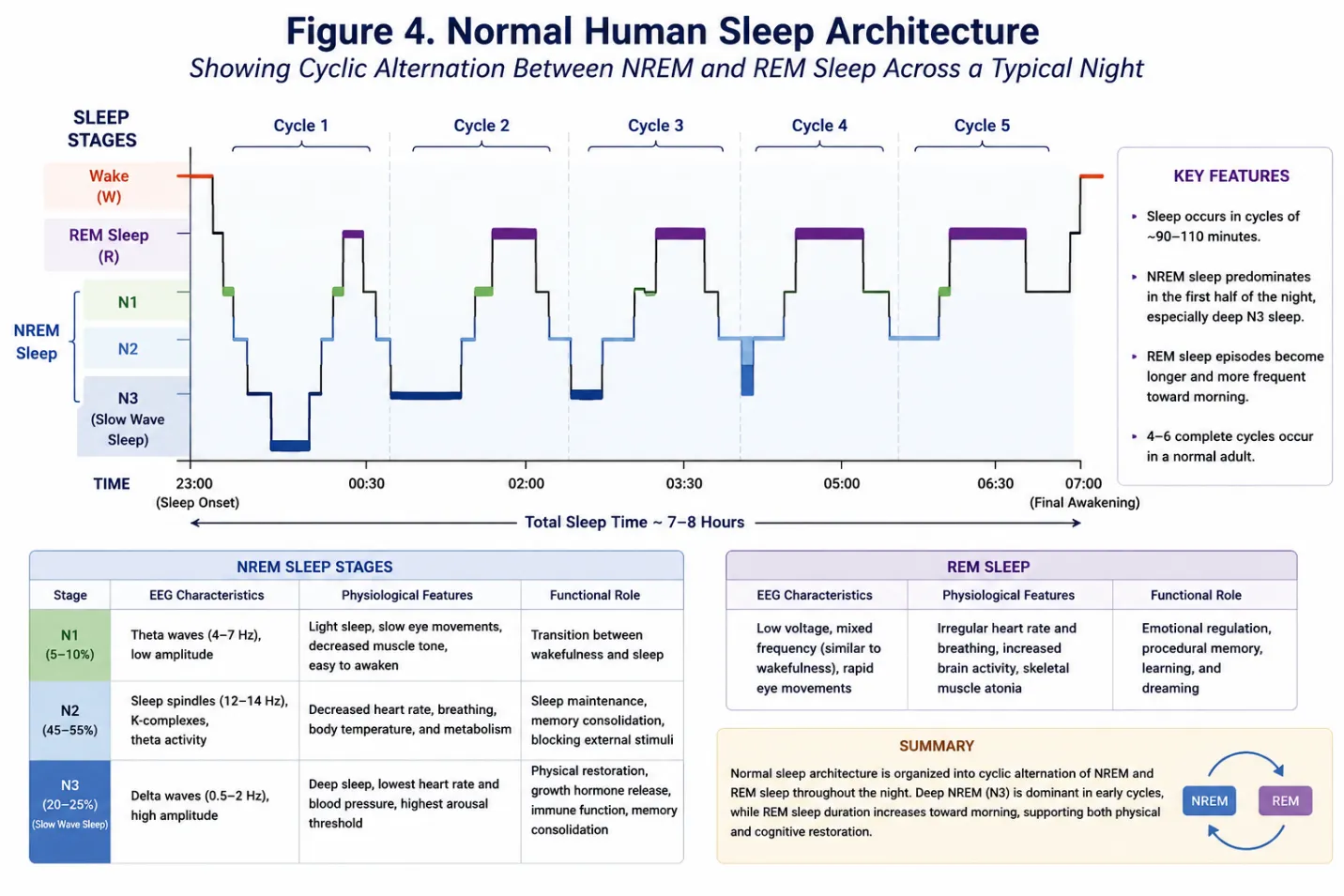
Figure4. Normal Human Sleep Architecture
3. Pharmacological Profile of Quetiapine
3.1 Chemical Characteristics and Classification
Quetiapine is a second-generation (atypical) antipsychotic belonging to the dibenzothiazepine class of psychotropic agents. Since its introduction into clinical practice, quetiapine has become an established therapeutic option for the management of schizophrenia, bipolar disorder, and, in several countries, as an adjunctive treatment for major depressive disorder. Compared with first-generation antipsychotics, quetiapine demonstrates a broader receptor-binding profile and a lower propensity to produce extrapyramidal symptoms at therapeutic doses. Its distinctive pharmacological characteristics also account for its well-recognized sedative properties, which have generated considerable interest regarding its influence on sleep physiology. Chemically, quetiapine is designated by the International Union of Pure and Applied Chemistry (IUPAC) as 2-[2-(4-dibenzo[b,f][1,4]thiazepin-11-ylpiperazin-1-yl)ethoxy]ethanol. In clinical practice, it is administered as quetiapine fumarate, a fumarate salt that improves chemical stability and oral pharmaceutical formulation. Following oral administration, quetiapine fumarate rapidly dissociates, releasing the active quetiapine molecule responsible for its pharmacological activity. The molecular formula of quetiapine is C₂₁H₂₅N₃O₂S, whereas quetiapine fumarate has the molecular formula C₄₂H₅₀N₆O₄S₂·C₄H₄O₄. The molecular weight of quetiapine free base is approximately 383.5 g/mol.
Structurally, quetiapine contains a tricyclic dibenzothiazepine nucleus linked to a piperazine ring through an ethoxyethanol side chain. This structural arrangement contributes to its affinity for multiple neurotransmitter receptors, including histamine H₁, serotonin 5-HT₂A, dopamine D₂, and α₁-adrenergic receptors. Unlike highly selective receptor ligands, quetiapine exhibits a multireceptor binding profile, which forms the pharmacological basis for both its therapeutic efficacy and its characteristic sedative effects. From a pharmacological perspective, quetiapine is classified as an atypical antipsychotic because it produces antipsychotic activity with a comparatively lower risk of extrapyramidal adverse effects than most first-generation antipsychotics. This favorable neurological profile is attributed primarily to relatively transient dopamine D₂ receptor occupancy together with prominent antagonism of serotonin 5-HT₂A receptors. In addition, potent histamine H₁ receptor antagonism contributes substantially to sedation and facilitation of sleep initiation, while α₁-adrenergic receptor blockade may further reduce central arousal. These pharmacodynamic characteristics distinguish quetiapine from conventional antipsychotic agents and explain its unique clinical profile. Several physicochemical properties influence the pharmacological behavior of quetiapine. The drug exhibits adequate lipophilicity, enabling efficient penetration across the blood–brain barrier and access to central nervous system receptors. It is well absorbed following oral administration and is available in both immediate-release (IR) and extended-release (XR) formulations, allowing flexibility in clinical dosing according to therapeutic requirements. Quetiapine undergoes extensive hepatic metabolism, predominantly through cytochrome P450 3A4 (CYP3A4), resulting in the formation of several metabolites, including the pharmacologically active metabolite norquetiapine. These physicochemical and pharmacokinetic characteristics contribute to its onset of action, receptor interactions, and overall therapeutic profile. The chemical structure, classification, and physicochemical properties of quetiapine collectively provide the foundation for understanding its complex pharmacology. These characteristics influence receptor affinity, central nervous system distribution, metabolic transformation, and ultimately the mechanisms through which quetiapine promotes sleep. A detailed discussion of its pharmacodynamic and pharmacokinetic properties is therefore essential for understanding the neurobiological basis of quetiapine-induced sleep promotion presented in the following sections.
Table 6. Chemical and Physicochemical Characteristics of Quetiapine
|
Parameter |
Description |
|
Generic name |
Quetiapine |
|
Pharmaceutical form |
Quetiapine fumarate |
|
Chemical class |
Dibenzothiazepine derivative |
|
Therapeutic class |
Second-generation (atypical) antipsychotic |
|
IUPAC name |
2-[2-(4-Dibenzo[b,f][1,4]thiazepin-11-ylpiperazin-1-yl)ethoxy]ethanol |
|
Molecular formula (free base) |
C₂₁H₂₅N₃O₂S |
|
Approximate molecular weight |
383.5 g/mol |
|
Route of administration |
Oral (Immediate-release and Extended-release formulations) |
|
Blood–brain barrier penetration |
High |
|
Primary metabolism |
Hepatic (predominantly CYP3A4) |
|
Major active metabolite |
Norquetiapine |
3.2 Pharmacodynamics
Pharmacodynamics describes the biochemical and physiological effects of a drug on the body and the molecular mechanisms through which these effects are produced. The pharmacological activity of quetiapine is distinguished by its interaction with multiple neurotransmitter receptors rather than selective modulation of a single target. This broad receptor-binding profile underlies its antipsychotic, mood-stabilizing, antidepressant, anxiolytic, and sedative properties. The clinical response to quetiapine is therefore determined by the combined influence of several receptor systems, with the relative contribution of each receptor varying according to the administered dose.
3.2.1 Mechanism of Action
Unlike first-generation antipsychotics, whose therapeutic efficacy primarily depends on sustained dopamine D₂ receptor blockade, quetiapine exerts its pharmacological effects through simultaneous modulation of dopaminergic, serotonergic, histaminergic, adrenergic, and muscarinic neurotransmission. Its antipsychotic efficacy is mainly attributed to antagonism of dopamine D₂ receptors together with potent blockade of serotonin 5-HT₂A receptors. The relatively transient occupancy of D₂ receptors allows effective control of psychotic symptoms while reducing the likelihood of extrapyramidal adverse effects compared with many conventional antipsychotics. Quetiapine also demonstrates high affinity for histamine H₁ receptors, which is considered the principal mechanism responsible for its pronounced sedative effects. Antagonism of H₁ receptors suppresses histaminergic arousal pathways originating from the tuberomammillary nucleus, thereby facilitating sleep initiation and reducing wakefulness. Additional antagonism of α₁-adrenergic receptors decreases central sympathetic activity and contributes to sedation and reduced physiological arousal. Furthermore, the active metabolite norquetiapine exhibits pharmacological properties distinct from the parent compound, including inhibition of the norepinephrine transporter (NET) and partial agonism at serotonin 5-HT₁A receptors, mechanisms that may contribute to antidepressant activity and overall therapeutic benefit.
3.2.2 Multireceptor Antagonism
A defining characteristic of quetiapine is its multireceptor pharmacology. Rather than acting on a single neurotransmitter system, quetiapine interacts with several receptor populations that collectively influence psychosis, mood, cognition, and sleep. Potent antagonism of histamine H₁ receptors accounts for the early sedative effect observed after administration, whereas serotonin 5-HT₂A receptor blockade contributes to antipsychotic efficacy, improvement of sleep continuity, and reduction of extrapyramidal symptoms associated with dopamine receptor antagonism. Dopamine D₂ receptor antagonism provides therapeutic control of positive psychotic symptoms, while α₁-adrenergic receptor blockade contributes to reduced autonomic arousal and may facilitate sleep initiation. Quetiapine exhibits relatively low affinity for muscarinic cholinergic receptors, although mild anticholinergic effects may occur in some individuals, particularly through the activity of norquetiapine. The interaction among these receptor systems explains why quetiapine demonstrates a broad spectrum of clinical effects extending beyond psychosis. Importantly, the sedative effects observed at lower doses are largely mediated by receptors other than dopamine D₂, emphasizing that quetiapine-induced sleep promotion is mechanistically distinct from its antipsychotic activity.
3.2.3 Dose-Dependent Receptor Occupancy
The pharmacological profile of quetiapine changes substantially with increasing dose because receptor occupancy is dose dependent. At lower doses, quetiapine predominantly occupies histamine H₁ and α₁-adrenergic receptors, resulting in marked sedation and facilitation of sleep with relatively limited dopamine D₂ receptor blockade. As the dose increases, occupancy of serotonin 5-HT₂A receptors becomes more pronounced, followed by greater interaction with dopamine D₂ receptors at doses typically used for the treatment of schizophrenia and bipolar disorder. This progressive pattern of receptor engagement explains why the clinical effects of quetiapine vary across different therapeutic dose ranges. Although receptor occupancy generally increases with dose, individual variability in absorption, hepatic metabolism, age, concomitant medications, and genetic differences affecting CYP3A4 activity may influence receptor exposure and clinical response. Consequently, therapeutic dosing should always be individualized according to the patient's clinical condition, treatment goals, and tolerability.
3.2.4 Therapeutic Pharmacological Effects
The diverse receptor interactions of quetiapine produce multiple clinically important therapeutic effects. Dopamine D₂ and serotonin 5-HT₂A receptor antagonism provide antipsychotic efficacy by reducing positive symptoms such as hallucinations and delusions while minimizing the risk of extrapyramidal symptoms compared with many first-generation antipsychotics. Modulation of serotonergic and noradrenergic neurotransmission, particularly through norquetiapine, contributes to mood stabilization and antidepressant activity observed in bipolar disorder and major depressive disorder. From the perspective of sleep regulation, antagonism of histamine H₁ receptors represents the most significant pharmacological mechanism underlying quetiapine-induced sedation. Additional blockade of serotonin 5-HT₂A and α₁-adrenergic receptors further reduces physiological arousal and may improve sleep continuity in susceptible individuals. However, these beneficial effects should be interpreted within the broader context of the drug's overall safety profile, as excessive sedation, orthostatic hypotension, and metabolic adverse effects may limit long-term clinical use. Therefore, the therapeutic actions of quetiapine arise from the integrated modulation of multiple neurotransmitter systems rather than from a single pharmacological mechanism, making it one of the most pharmacodynamically complex agents among second-generation antipsychotics.
3.4 Receptor Binding Profile
The pharmacological profile of quetiapine is characterized by its ability to interact with multiple neurotransmitter receptors that regulate psychosis, mood, cognition, and sleep. Unlike highly selective receptor ligands, quetiapine exhibits a broad receptor-binding spectrum, and its therapeutic as well as adverse effects result from the combined modulation of several neurotransmitter systems. The degree of receptor occupancy varies with dose, plasma concentration, and individual pharmacokinetic characteristics, making receptor-binding affinity a key determinant of its clinical response. This multireceptor pharmacology explains why quetiapine possesses antipsychotic, mood-stabilizing, anxiolytic, antidepressant, and sedative properties within different therapeutic dose ranges.
3.4.1 Histamine H₁ Receptors
Quetiapine exhibits very high affinity for histamine H₁ receptors, making this receptor one of its principal pharmacological targets. Histaminergic neurons arising from the tuberomammillary nucleus of the posterior hypothalamus play a critical role in maintaining cortical arousal and wakefulness. Antagonism of H₁ receptors suppresses histaminergic neurotransmission, resulting in decreased alertness, facilitation of sleep onset, and increased subjective sleepiness. Because substantial H₁ receptor occupancy occurs even at relatively low doses, sedation is often observed before significant dopamine D₂ receptor blockade develops. This receptor interaction represents the primary neuropharmacological mechanism responsible for the sleep-promoting effects of quetiapine and explains its frequent clinical use in patients experiencing insomnia associated with psychiatric disorders.
3.4.2 Serotonin (5-HT₂A and 5-HT₂C) Receptors
Quetiapine demonstrates high affinity for serotonin 5-HT₂A receptors and comparatively lower affinity for 5-HT₂C receptors. Blockade of 5-HT₂A receptors enhances the balance between serotonergic and dopaminergic neurotransmission, thereby contributing to antipsychotic efficacy while reducing the risk of extrapyramidal symptoms associated with dopamine receptor antagonism. In addition, inhibition of cortical 5-HT₂A signaling has been associated with improved sleep continuity, decreased nocturnal arousal, and stabilization of sleep architecture. Although antagonism of 5-HT₂C receptors is less pronounced, this receptor may influence appetite regulation, emotional processing, and metabolic homeostasis. Together, serotonergic receptor modulation contributes to both the therapeutic efficacy and the sleep-related benefits of quetiapine.
3.4.3 Dopamine (D₁ and D₂) Receptors
The antipsychotic activity of quetiapine is primarily mediated through antagonism of dopamine D₂ receptors within the mesolimbic pathway. Compared with many first-generation antipsychotics, quetiapine exhibits relatively transient D₂ receptor occupancy, allowing effective management of psychotic symptoms while minimizing extrapyramidal adverse effects. At lower doses, D₂ receptor occupancy remains modest, indicating that sedation is largely independent of dopamine blockade. As the administered dose increases, D₂ receptor occupancy also increases, providing greater therapeutic efficacy in schizophrenia and bipolar disorder. Quetiapine possesses relatively low affinity for dopamine D₁ receptors, and current evidence suggests that D₁ receptor interactions contribute minimally to its overall pharmacological profile compared with D₂ receptor modulation.
3.4.4 α₁- and α₂-Adrenergic Receptors
Quetiapine antagonizes both α₁- and α₂-adrenergic receptors, although its affinity is considerably greater for α₁ receptors. Blockade of α₁ receptors reduces sympathetic nervous system activity, producing vasodilation, decreased physiological arousal, and clinically significant sedation. This mechanism contributes to improved sleep initiation but may also explain adverse effects such as orthostatic hypotension, dizziness, and transient reductions in blood pressure during treatment initiation or dose escalation. Antagonism of α₂-adrenergic receptors may modestly influence noradrenergic neurotransmission and contribute to anxiolytic and antidepressant effects, particularly through interactions involving the active metabolite norquetiapine.
3.4.5 Muscarinic Receptors
Compared with several other atypical antipsychotics, quetiapine demonstrates relatively low affinity for muscarinic cholinergic receptors. Consequently, direct anticholinergic adverse effects are generally less prominent with the parent drug. Nevertheless, mild manifestations such as dry mouth, constipation, blurred vision, or urinary retention may occur in susceptible individuals, particularly during prolonged therapy. The active metabolite norquetiapine exhibits greater muscarinic receptor affinity than quetiapine itself and may contribute to these effects. Current evidence indicates that muscarinic receptor antagonism plays only a limited role in the sleep-promoting properties of quetiapine.
3.4.6 Clinical Relevance of Receptor Affinity
The receptor-binding profile of quetiapine provides the pharmacological basis for its broad therapeutic spectrum. High affinity for histamine H₁ receptors is primarily responsible for its sedative and sleep-promoting actions, whereas antagonism of serotonin 5-HT₂A receptors enhances antipsychotic efficacy and may improve sleep continuity. Dopamine D₂ receptor antagonism remains essential for controlling psychotic symptoms while relatively transient receptor occupancy contributes to a lower incidence of extrapyramidal symptoms compared with many first-generation antipsychotics. Blockade of α₁-adrenergic receptors further facilitates sedation but may increase the risk of orthostatic hypotension, whereas muscarinic receptor interactions contribute minimally to therapeutic sleep induction. Collectively, these receptor interactions explain the dose-dependent pharmacological profile of quetiapine and provide the mechanistic foundation for its clinical use in psychiatric disorders associated with disturbed sleep.
Table 8. Receptor Binding Profile of Quetiapine and Associated Clinical Significance
|
Receptor |
Relative Affinity of Quetiapine |
Primary Pharmacological Action |
Clinical Significance |
|
Histamine H₁ |
Very High |
Competitive antagonism |
Produces sedation, facilitates sleep initiation, reduces wakefulness, and contributes substantially to the sleep-promoting effects of quetiapine. |
|
Serotonin 5-HT₂A |
High |
Antagonism |
Improves antipsychotic efficacy, reduces extrapyramidal symptoms, enhances sleep continuity, and may decrease nocturnal arousals. |
|
Serotonin 5-HT₂C |
Moderate |
Antagonism |
May influence mood regulation, appetite, and metabolic function; contributes minimally to sleep promotion. |
|
Dopamine D₂ |
Moderate (rapid dissociation) |
Antagonism |
Responsible for antipsychotic efficacy while maintaining a relatively lower risk of extrapyramidal adverse effects because of transient receptor occupancy. |
|
Dopamine D₁ |
Low |
Weak antagonism |
Limited contribution to the overall therapeutic effects of quetiapine. |
|
α₁-Adrenergic |
High |
Antagonism |
Reduces sympathetic arousal, promotes sedation, and may cause orthostatic hypotension and dizziness. |
|
α₂-Adrenergic |
Moderate |
Antagonism |
May modestly influence noradrenergic neurotransmission and contribute to anxiolytic and antidepressant effects. |
|
Muscarinic (M₁–M₅) |
Low (parent drug) |
Weak antagonism |
Minor contribution to anticholinergic effects; limited role in sleep promotion. |
|
Norepinephrine Transporter (NET)* |
High (Norquetiapine) |
Inhibition |
Contributes to antidepressant activity and may improve overall mood and daytime functioning. |
|
Serotonin 5-HT₁A* |
Partial agonist (Norquetiapine) |
Partial agonism |
Associated with antidepressant and anxiolytic effects; may indirectly improve sleep quality by reducing anxiety and depressive symptoms. |
Abbreviations: H₁, histamine H₁ receptor; 5-HT, serotonin receptor; D₁/D₂, dopamine receptors; α₁/α₂, alpha-adrenergic receptors; NET, norepinephrine transporter.
*These pharmacological actions are mediated primarily by norquetiapine, the major active metabolite of quetiapine, rather than the parent compound.
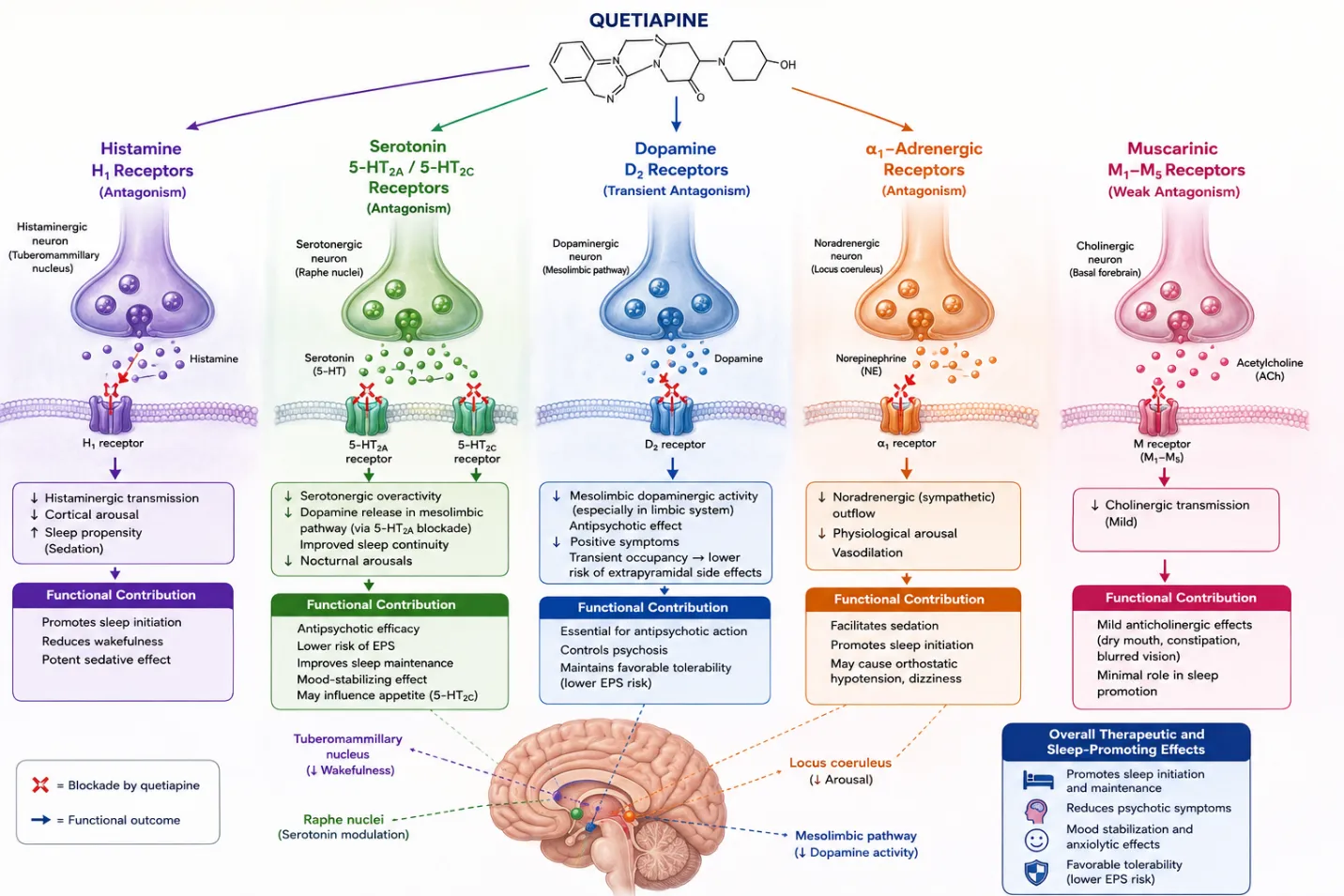
Figure 8. Major Neurotransmitter Receptors Targeted by Quetiapine and Their Functional Contribution to Therapeutic and Sleep-Promoting Effects
4. Neuropharmacological Mechanisms Underlying the Sleep-Promoting Effects of Quetiapine
The sleep-promoting effects of quetiapine are primarily a consequence of its multireceptor pharmacology, involving coordinated modulation of histaminergic, serotonergic, adrenergic, dopaminergic, and metabolite-mediated pathways. Unlike classical hypnotics that directly enhance GABAergic inhibition, quetiapine facilitates sleep by reducing the activity of multiple wake-promoting neurotransmitter systems, thereby shifting the neurobiological balance toward a sleep-preferential state. This indirect mechanism explains both its sedative properties and its variability in sleep response across individuals.
4.1 Histamine H₁ receptor antagonism and sleep initiation
Among all receptor targets, antagonism of histamine H₁ receptors is considered the most important mechanism responsible for the acute sedative effect of quetiapine. Histaminergic neurons in the tuberomammillary nucleus of the posterior hypothalamus play a central role in maintaining cortical arousal and wakefulness. During normal wake states, histamine release promotes alertness, attention, and behavioral activation through widespread projections to the cortex and subcortical structures. Quetiapine exhibits high affinity for H₁ receptors, and even at relatively low doses it significantly reduces histaminergic signaling. This leads to decreased cortical activation and a rapid reduction in subjective alertness, facilitating sleep initiation. This mechanism also explains why sedation is often observed at doses lower than those required for antipsychotic efficacy.
4.2 Serotonin 5-HT₂A receptor blockade and sleep architecture modulation
Blockade of serotonin 5-HT₂A receptors contributes to improvement in sleep continuity and stabilization of sleep architecture. The serotonergic system has a complex role in sleep regulation, influencing cortical excitability and transitions between sleep stages. Antagonism of 5-HT₂A receptors reduces cortical hyperarousal and decreases nocturnal awakenings, thereby supporting more consolidated sleep. This mechanism is particularly relevant in psychiatric populations, where serotonergic dysregulation is commonly associated with fragmented sleep patterns. In addition, 5-HT₂A blockade indirectly supports NREM sleep stability and may reduce REM-related sleep disturbances in certain clinical conditions.
4.3 α₁-adrenergic receptor antagonism and reduction of physiological arousal
Quetiapine also antagonizes α₁-adrenergic receptors, contributing to a reduction in central and peripheral sympathetic tone. This results in decreased physiological arousal, reduced vigilance, and facilitation of sleep onset. The adrenergic system is a key component of the ascending arousal network, and its inhibition supports transition from wakefulness to sleep. However, this mechanism is also responsible for clinically relevant adverse effects such as orthostatic hypotension and dizziness, particularly during dose initiation or titration. Despite these limitations, α₁ blockade plays an important complementary role in the overall sedative profile of quetiapine.
4.4 Dopamine D₂ receptor modulation and indirect effects on sleep
Dopamine D₂ receptor antagonism contributes primarily to the antipsychotic effects of quetiapine, but its role in sleep regulation is indirect. Dopaminergic pathways are strongly associated with wakefulness, motivation, and reward-driven behavior. By modulating mesolimbic dopamine activity, quetiapine reduces psychotic symptoms, agitation, and cognitive overactivation, all of which can secondarily improve sleep quality. Importantly, quetiapine exhibits relatively transient D₂ receptor occupancy compared to typical antipsychotics, which may reduce motor side effects while still providing therapeutic benefit without strongly disrupting sleep architecture.
4.5 Role of norquetiapine in sleep regulation
Norquetiapine, the active metabolite of quetiapine, adds further complexity to its neuropharmacological profile. It inhibits the norepinephrine transporter (NET), leading to increased synaptic norepinephrine levels in certain brain regions, and acts as a partial agonist at 5-HT₁A receptors. While these actions are more strongly associated with antidepressant effects, they indirectly influence sleep by reducing depressive and anxiety symptoms that commonly contribute to insomnia. By improving mood regulation and emotional stability, norquetiapine may enhance sleep continuity and subjective sleep quality, particularly in patients with comorbid mood disorders.
Integrated mechanism of sleep promotion
The sleep-promoting effects of quetiapine cannot be attributed to a single receptor system but instead arise from the integrated suppression of multiple arousal pathways. Histaminergic inhibition initiates sedation, serotonergic blockade stabilizes sleep architecture, adrenergic antagonism reduces physiological arousal, and dopaminergic modulation decreases cognitive and emotional overactivation. Norquetiapine further supports this system by improving affective symptoms that interfere with sleep. Together, these converging mechanisms shift the brain from a wake-promoting state toward a sleep-facilitating neurochemical environment. This multimodal action explains why quetiapine is effective in improving sleep in patients with psychiatric disorders, although its use as a primary hypnotic agent remains limited due to metabolic and cardiovascular side effects. of quetiapine, adds further complexity to its neuropharmacological profile. It inhibits the norepinephrine transporter (NET), leading to increased synaptic norepinephrine levels in certain brain regions, and acts as a partial agonist at 5-HT₁A receptors. While these actions are more strongly associated with antidepressant effects, they indirectly influence sleep by reducing depressive and anxiety symptoms that commonly contribute to insomnia. By improving mood regulation and emotional stability, norquetiapine may enhance sleep continuity and subjective sleep quality, particularly in patients with comorbid mood disorders.
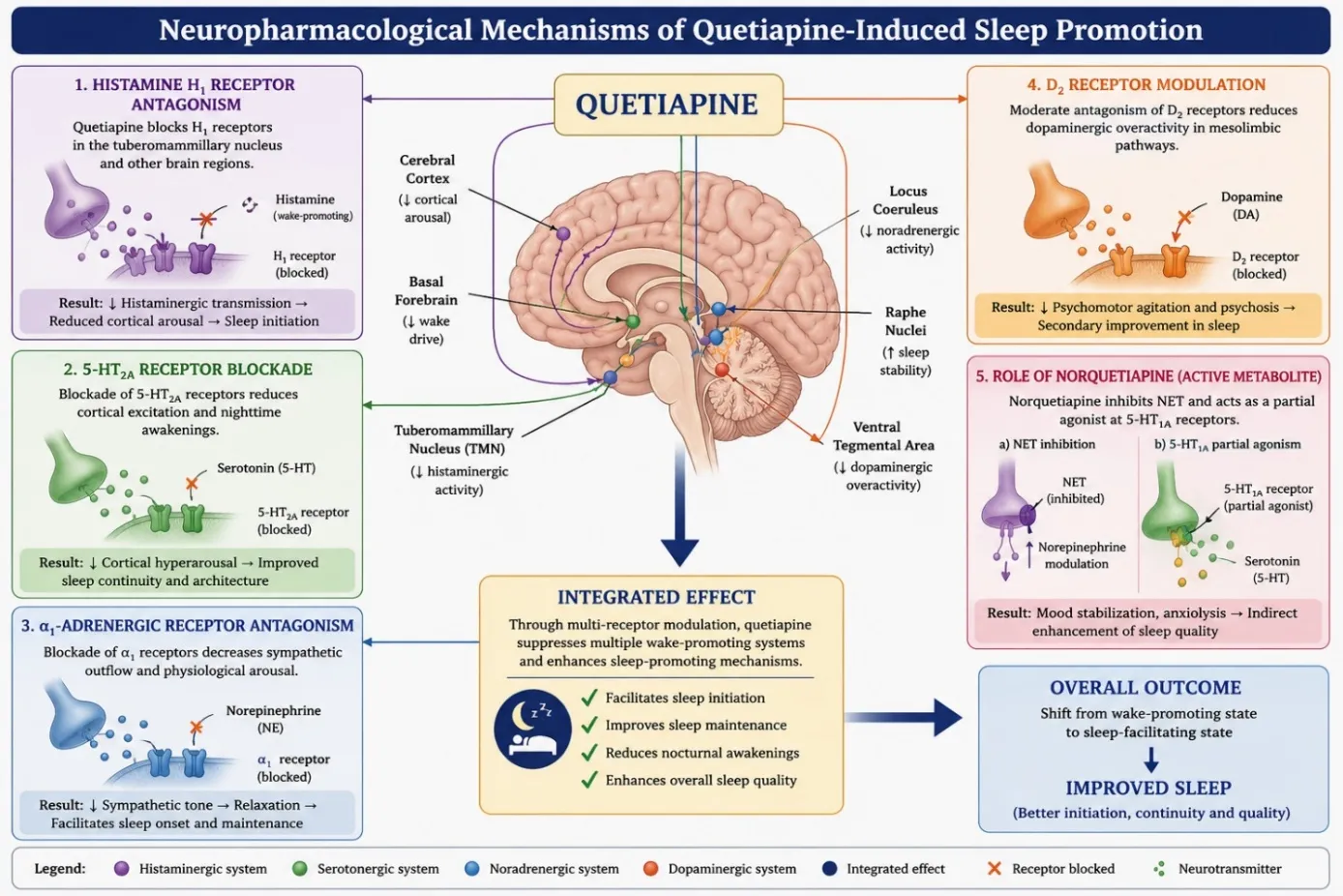
Figure 9. Neuropharmacological Mechanisms Underlying the Sleep-Promoting Effects of Quetiapine
5. Dose-Dependent Sedative Effects of Quetiapine
The sedative effects of quetiapine are highly dose dependent and reflect its differential affinity for multiple neurotransmitter receptors. Unlike many psychotropic medications whose pharmacological actions increase proportionally with dose, quetiapine demonstrates a characteristic shift in receptor engagement as plasma concentrations rise. At lower doses, the drug predominantly occupies histamine H₁ and α₁-adrenergic receptors, resulting in pronounced sedation with relatively limited dopamine D₂ receptor blockade. As the dose increases, serotonin 5-HT₂A and dopamine D₂ receptor occupancy progressively become more prominent, leading to antipsychotic and mood-stabilizing effects that extend beyond sedation. Consequently, the clinical response to quetiapine varies substantially across different therapeutic dose ranges. Low-dose quetiapine is characterized primarily by its potent antihistaminic activity. Histamine H₁ receptor antagonism rapidly suppresses the activity of wake-promoting neurons originating from the tuberomammillary nucleus, thereby reducing cortical arousal and facilitating sleep initiation. Concurrent antagonism of α₁-adrenergic receptors further decreases sympathetic nervous system activity, promoting relaxation and reducing physiological hyperarousal. Because dopamine D₂ receptor occupancy remains relatively low at these doses, sedation generally occurs without producing substantial extrapyramidal adverse effects. This pharmacological profile explains why low-dose quetiapine has frequently been prescribed in clinical practice for patients experiencing insomnia associated with psychiatric disorders, although such use is considered off-label in many countries. As the administered dose increases, quetiapine begins to exhibit greater occupancy of serotonin 5-HT₂A receptors, enhancing antipsychotic efficacy while simultaneously improving sleep continuity. Antagonism of 5-HT₂A receptors has been associated with reduced nocturnal awakenings and stabilization of sleep architecture, complementing the sedative effects mediated by H₁ receptor blockade. During this intermediate dose range, patients often experience both improved sleep and clinically significant benefits in mood, anxiety, or psychotic symptoms depending on the underlying disorder. Consequently, improvements in sleep may result not only from direct receptor-mediated sedation but also from successful treatment of psychiatric symptoms that interfere with normal sleep. At higher therapeutic doses, dopamine D₂ receptor antagonism becomes increasingly important. Greater D₂ receptor occupancy provides effective control of positive psychotic symptoms, including hallucinations and delusions, while the relatively rapid dissociation of quetiapine from D₂ receptors contributes to a lower incidence of extrapyramidal symptoms compared with many first-generation antipsychotics. Although sedation remains clinically apparent because H₁ receptor occupancy persists, the predominant therapeutic objective shifts from sleep promotion to the management of schizophrenia, bipolar disorder, and related psychiatric conditions. Thus, sedation becomes one component of a broader pharmacological profile rather than the principal therapeutic effect. Individual variability significantly influences the magnitude of quetiapine-induced sedation. Age, hepatic function, body composition, genetic variation in CYP3A4 activity, concomitant medications, and underlying psychiatric illness all affect systemic drug exposure and receptor occupancy. Older adults frequently exhibit greater sensitivity to sedative effects because of altered pharmacokinetics and increased central nervous system susceptibility. Likewise, co-administration of other sedative agents, including benzodiazepines, opioids, alcohol, or antihistamines, may potentiate central nervous system depression and increase the risk of excessive daytime somnolence, falls, or cognitive impairment. Although sedation is often therapeutically beneficial in patients with insomnia associated with psychiatric disorders, it may also produce undesirable consequences. Excessive daytime sleepiness, impaired psychomotor performance, reduced attention, dizziness, and orthostatic hypotension are among the most frequently reported adverse effects. Long-term treatment is additionally associated with metabolic complications, including weight gain, dyslipidaemia, and impaired glucose metabolism, which should be considered when evaluating the overall risk–benefit profile of quetiapine. For these reasons, major clinical guidelines generally do not recommend quetiapine as a first-line treatment for primary insomnia in individuals without an approved psychiatric indication. Overall, the sedative effects of quetiapine arise from a dynamic interaction between receptor affinity and dose-dependent receptor occupancy. Histamine H₁ receptor antagonism predominates at lower doses, whereas serotonergic and dopaminergic mechanisms become increasingly important as the dose escalates. Understanding this pharmacological transition is essential for optimizing therapeutic efficacy, minimizing adverse effects, and interpreting the clinical evidence regarding the sleep-promoting properties of quetiapine.
Table 11. Dose-Dependent Receptor Engagement and Predominant Clinical Effects of Quetiapine
|
Dose Category |
Predominant Neuropharmacological Targets |
Primary Pharmacological Effects |
Major Clinical Outcomes |
|
Low dose (commonly ≤100 mg/day*) |
Histamine H₁ receptors, α₁-adrenergic receptors |
Marked antihistaminic activity with reduced physiological arousal |
Sedation, facilitation of sleep initiation, reduced wakefulness, improvement in insomnia symptoms (particularly in patients with psychiatric disorders) |
|
Moderate dose (approximately 150–300 mg/day*) |
Histamine H₁, serotonin 5-HT₂A, α₁-adrenergic receptors; increasing dopamine D₂ receptor engagement |
Combined sedative, anxiolytic, antidepressant, and antipsychotic actions |
Improved sleep continuity, mood stabilization, reduction in anxiety symptoms, therapeutic benefit in bipolar depression and other mood disorders |
|
High dose (approximately 400–800 mg/day*) |
Dopamine D₂ receptors, serotonin 5-HT₂A receptors, with persistent H₁ receptor antagonism |
Predominantly antipsychotic activity while maintaining sedative properties |
Control of psychotic symptoms in schizophrenia and bipolar disorder, with sedation remaining a common adverse effect |
Abbreviations: H₁, histamine H₁ receptor; 5-HT₂A, serotonin 5-hydroxytryptamine receptor subtype 2A; D₂, dopamine D₂ receptor.
*The dose ranges shown are approximate clinical therapeutic ranges commonly described in the literature. Receptor occupancy does not change at fixed dose thresholds and varies among individuals according to pharmacokinetic factors (e.g., CYP3A4 metabolism), age, hepatic function, concomitant medications, and the formulation used (immediate-release vs. extended-release). Therefore, these ranges should be interpreted as general clinical guidance rather than absolute pharmacological cut-offs.
6. Clinical Evidence for the Sleep-Promoting Effects of Quetiapine
The sleep-promoting effects of quetiapine have been investigated in a variety of clinical settings, including schizophrenia, bipolar disorder, major depressive disorder, generalized anxiety disorder, and insomnia associated with psychiatric illness. Although quetiapine is primarily approved as an atypical antipsychotic, numerous clinical studies have consistently reported improvements in subjective and objective measures of sleep following treatment. These benefits are generally attributed to its combined antagonism of histamine H₁, serotonin 5-HT₂A, and α₁-adrenergic receptors, together with the indirect effects of symptom control on sleep quality. In patients with schizophrenia, sleep disturbances are highly prevalent and are frequently characterized by prolonged sleep latency, fragmented sleep, reduced sleep efficiency, and abnormalities in both NREM and REM sleep. Clinical trials have shown that quetiapine treatment is associated with improvements in sleep continuity, increased total sleep time, reduced nocturnal awakenings, and enhanced subjective sleep quality. These improvements occur alongside reductions in psychotic symptoms, making it difficult to distinguish direct pharmacological sedation from secondary improvements resulting from effective disease control. Nevertheless, polysomnographic studies indicate that quetiapine can positively influence sleep architecture independent of its antipsychotic efficacy.
Patients with bipolar disorder commonly experience significant sleep disruption during both manic and depressive episodes. Restoration of normal sleep is considered an important therapeutic objective because disturbed sleep itself may precipitate mood relapse. Clinical evidence suggests that quetiapine improves sleep onset, decreases nighttime awakenings, and enhances overall sleep quality in both bipolar depression and maintenance therapy. Improvement in sleep frequently parallels stabilization of mood symptoms, indicating that both receptor-mediated sedation and mood regulation contribute to the overall therapeutic response.
Quetiapine has also demonstrated beneficial effects on sleep in individuals with major depressive disorder (MDD), particularly when used as an adjunctive treatment. Many patients with depression experience insomnia characterized by difficulty initiating sleep, frequent awakenings, or early morning awakening. By combining sedative receptor blockade with the antidepressant actions of its active metabolite, norquetiapine, quetiapine may improve both depressive symptoms and sleep quality. Clinical studies have reported reductions in insomnia severity together with improvements in subjective sleep satisfaction, although daytime somnolence remains a commonly reported adverse effect.
In patients with generalized anxiety disorder (GAD) and related anxiety disorders, excessive physiological arousal frequently interferes with normal sleep. Quetiapine has been shown to reduce anxiety symptoms while simultaneously improving sleep initiation and maintenance. These effects are likely mediated through suppression of central arousal pathways together with improvement of anxiety-related hypervigilance. However, because of concerns regarding metabolic adverse effects and long-term safety, quetiapine is generally reserved for carefully selected patients when alternative therapeutic options are unsuitable.
The use of quetiapine for primary insomnia remains controversial. Although several small clinical studies have demonstrated improvements in sleep latency and subjective sleep quality, the available evidence is limited by relatively small sample sizes, short treatment durations, and inconsistent study methodologies. Current clinical practice guidelines generally advise against the routine use of quetiapine solely for the treatment of primary insomnia because the potential risks, including weight gain, metabolic abnormalities, excessive daytime sedation, and cardiovascular adverse effects, may outweigh the expected benefits in individuals without an approved psychiatric indication.
Systematic reviews and meta-analyses generally conclude that quetiapine improves several clinically relevant sleep outcomes, particularly in patients with underlying psychiatric disorders. Reported benefits include shorter sleep latency, increased total sleep time, improved sleep efficiency, fewer nocturnal awakenings, and better overall subjective sleep quality. However, the quality of available evidence varies considerably across different patient populations, and long-term randomized controlled trials evaluating sleep-specific outcomes remain relatively limited. Consequently, while the sleep-promoting effects of quetiapine are well recognized, current evidence supports its use primarily when sleep disturbance occurs in association with an established psychiatric disorder rather than as a routine hypnotic agent. Overall, the available clinical evidence indicates that quetiapine can substantially improve sleep in appropriately selected patients through both direct neuropharmacological mechanisms and indirect improvement of psychiatric symptoms. Nevertheless, treatment decisions should carefully balance the expected benefits against potential adverse effects, individual patient characteristics, and current evidence-based prescribing recommendations.
Table 12. Summary of Clinical Evidence Supporting the Sleep-Promoting Effects of Quetiapine Across Psychiatric Disorders
|
Psychiatric Disorder |
Common Sleep Disturbances |
Reported Effects of Quetiapine on Sleep |
Overall Clinical Evidence |
|
Schizophrenia |
Insomnia, prolonged sleep latency, fragmented sleep, reduced sleep efficiency |
Improved sleep initiation, increased total sleep time, reduced nocturnal awakenings, improved sleep continuity |
Multiple randomized clinical trials and polysomnographic studies support beneficial effects on sleep when used as part of antipsychotic therapy. |
|
Bipolar Disorder |
Reduced sleep during mania, insomnia during depressive episodes, circadian rhythm disturbances |
Improved sleep onset, better sleep maintenance, increased sleep duration, stabilization of sleep–wake rhythm |
Strong evidence from randomized controlled trials supports improvement in both mood symptoms and sleep quality. |
|
Major Depressive Disorder (Adjunctive Therapy) |
Difficulty initiating sleep, frequent nocturnal awakenings, early morning awakening |
Reduced insomnia severity, improved subjective sleep quality, enhanced sleep continuity |
Moderate to strong evidence supports improvement in sleep when quetiapine is used as adjunctive antidepressant therapy. |
|
Generalized Anxiety Disorder |
Hyperarousal, delayed sleep onset, poor sleep quality |
Reduced sleep latency, improved sleep maintenance, decreased anxiety-related sleep disturbance |
Randomized clinical trials demonstrate improvements in sleep, although long-term use is limited by tolerability concerns. |
|
Primary Insomnia (Off-label Use) |
Persistent insomnia without major psychiatric illness |
Short-term improvement in sleep initiation and subjective sleep quality reported in some studies |
Evidence remains limited and inconsistent; major clinical guidelines generally do not recommend routine use because potential risks may outweigh benefits. |
Abbreviations: RCT, randomized controlled trial.
Note: The strength of evidence summarized in this table reflects the overall consistency of published clinical studies and guideline recommendations rather than the findings of any single study. Quetiapine is approved for specific psychiatric disorders; its use for primary insomnia is generally off-label in many countries and should be considered only after careful evaluation of potential benefits and risks.
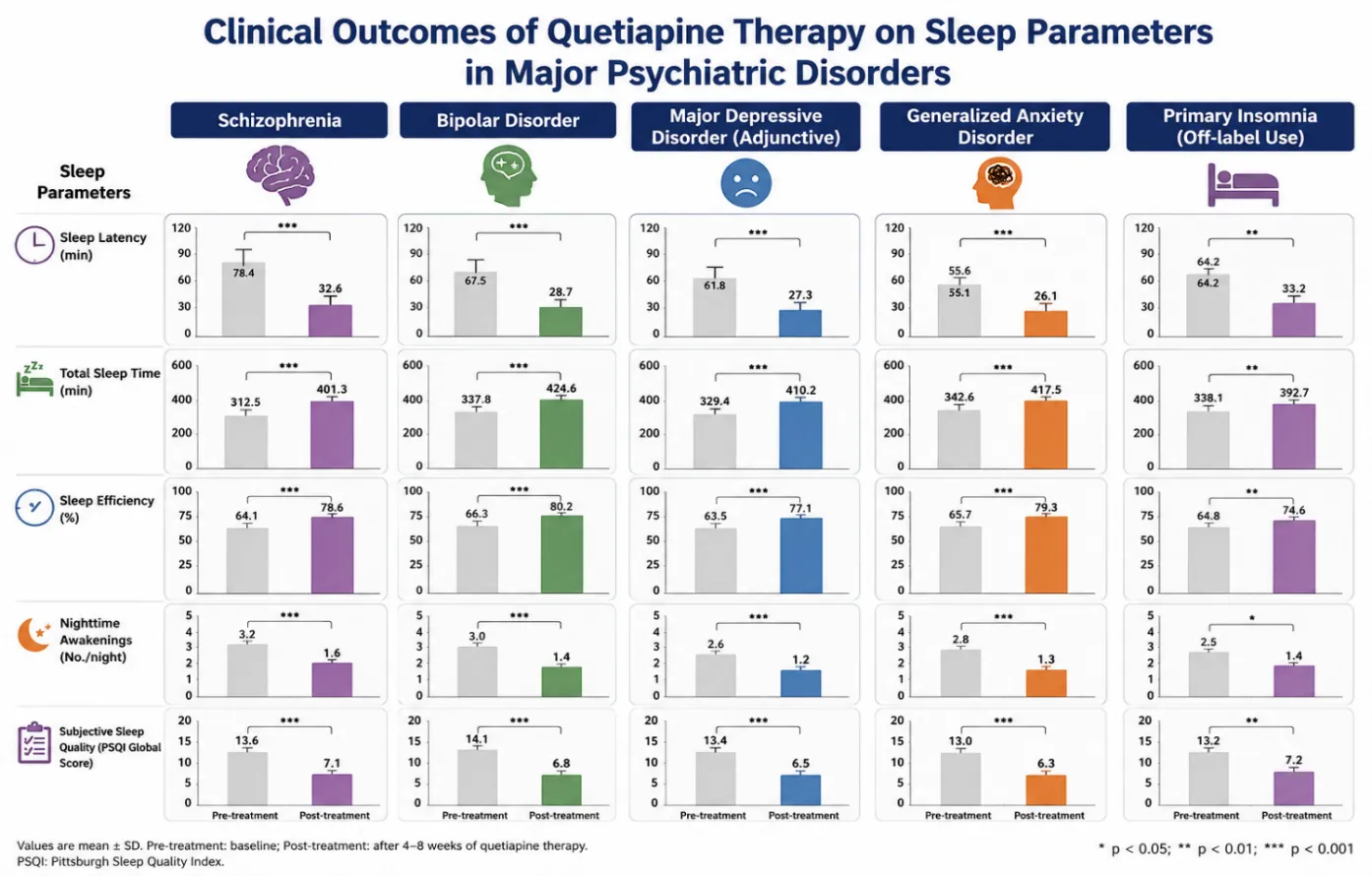
Figure 12. Clinical Outcomes of Quetiapine Therapy on Sleep Parameters Across Major Psychiatric Disorders
7. Safety Considerations and Clinical Limitations of Quetiapine for Sleep Promotion
Although quetiapine has demonstrated clinically meaningful sleep-promoting effects, its use should always be considered within the context of its overall safety profile. Unlike medications specifically developed for the treatment of insomnia, quetiapine is an atypical antipsychotic with a broad range of pharmacological actions that extend beyond sleep regulation. Consequently, the benefits of improved sleep must be carefully balanced against the potential for adverse effects, particularly during long-term therapy. Sedation is the most frequently reported adverse effect of quetiapine and is largely attributable to potent histamine H₁ receptor antagonism. While this property may be therapeutically beneficial in patients experiencing insomnia associated with psychiatric disorders, excessive sedation can impair daytime alertness, concentration, psychomotor performance, and occupational functioning. Older adults are particularly susceptible to excessive sedation because age-related pharmacokinetic and pharmacodynamic changes increase sensitivity to central nervous system depressants. Quetiapine is also associated with several metabolic adverse effects, including weight gain, dyslipidaemia, impaired glucose tolerance, and an increased risk of metabolic syndrome during prolonged treatment. These metabolic complications are clinically significant because they contribute to an elevated long-term risk of cardiovascular disease and type 2 diabetes mellitus. Therefore, regular monitoring of body weight, body mass index, fasting plasma glucose, glycated hemoglobin (HbA1c), and lipid profile is recommended during ongoing therapy, particularly in patients receiving moderate or high doses. Cardiovascular safety is another important consideration. Antagonism of α₁-adrenergic receptors may result in orthostatic hypotension, dizziness, and syncope, especially during treatment initiation or dose escalation. Quetiapine has also been associated with dose-related prolongation of the QT interval in susceptible individuals, although the overall risk is generally lower than that observed with certain other antipsychotic agents. Patients with pre-existing cardiovascular disease, electrolyte disturbances, or concomitant use of other QT-prolonging medications require careful clinical assessment before initiating treatment. Although quetiapine produces fewer extrapyramidal symptoms than many first-generation antipsychotics because of its relatively transient dopamine D₂ receptor occupancy, extrapyramidal adverse effects cannot be completely excluded. Akathisia, tremor, and mild parkinsonian symptoms have been reported, particularly at higher therapeutic doses. In addition, anticholinergic effects such as dry mouth, constipation, and blurred vision may occur, although these are generally less pronounced than with several other atypical antipsychotics. The use of quetiapine solely for the treatment of primary insomnia remains controversial. Several professional organizations, including sleep medicine and psychiatric guideline panels, advise against its routine off-label use for uncomplicated insomnia because current evidence does not demonstrate that the benefits consistently outweigh the potential risks. Instead, non-pharmacological interventions, particularly cognitive behavioral therapy for insomnia (CBT-I), remain the recommended first-line treatment for chronic insomnia, while pharmacological therapy should be individualized according to the patient's clinical condition and evidence-based indications. Appropriate patient selection is therefore essential when considering quetiapine for sleep-related symptoms. The medication may provide substantial benefit in individuals with schizophrenia, bipolar disorder, major depressive disorder, or anxiety disorders in whom insomnia represents a component of the underlying psychiatric illness. Conversely, the routine use of quetiapine as a hypnotic agent in otherwise healthy individuals should be approached with caution because of its metabolic, cardiovascular, and neurological adverse-effect profile. Overall, the available evidence indicates that quetiapine can effectively improve sleep when used for approved psychiatric indications; however, its safety profile necessitates careful clinical monitoring and individualized risk–benefit assessment. Rational prescribing should prioritize evidence-based indications, minimize unnecessary long-term exposure, and ensure regular monitoring for metabolic and cardiovascular complications throughout treatment.
8. Emerging Perspectives in Quetiapine Research
Continued research is needed to better define the role of quetiapine in the management of sleep disturbances across different clinical populations. Future randomized controlled trials should employ standardized objective measures, including polysomnography and actigraphy, together with validated patient-reported sleep outcomes to clarify the long-term effects of quetiapine on sleep architecture and overall sleep quality. Comparative studies evaluating quetiapine against approved insomnia therapies would further help determine its relative efficacy, safety, and appropriate place in clinical practice. Advances in neuropharmacology and precision medicine may provide opportunities to identify patient subgroups that derive the greatest benefit from quetiapine while minimizing treatment-related adverse effects. Greater understanding of receptor-specific mechanisms, the pharmacological contribution of norquetiapine, pharmacogenomic influences on therapeutic response, and long-term metabolic safety will improve individualized treatment strategies. In addition, the development of novel therapeutic agents capable of preserving the beneficial sleep-promoting properties of quetiapine while reducing metabolic and cardiovascular risks may represent an important future direction in psychopharmacological research.
CONCLUSION
Quetiapine is a second-generation antipsychotic with a distinctive multireceptor pharmacological profile that contributes to its clinically significant sleep-promoting effects. Unlike conventional hypnotic agents, its sedative action primarily results from potent antagonism of histamine H₁ receptors, while serotonin 5-HT₂A receptor blockade, α₁-adrenergic receptor antagonism, transient dopamine D₂ receptor modulation, and the pharmacological activity of norquetiapine collectively enhance sleep regulation. Through these complementary mechanisms, quetiapine facilitates sleep initiation, improves sleep continuity, and reduces nocturnal awakenings, particularly in patients with psychiatric disorders accompanied by insomnia. Current clinical evidence indicates that quetiapine improves several important sleep outcomes, including sleep latency, total sleep time, sleep efficiency, and subjective sleep quality in disorders such as schizophrenia, bipolar disorder, major depressive disorder, and generalized anxiety disorder. However, its clinical value should be interpreted within the context of its approved psychiatric indications rather than as a routine treatment for primary insomnia. The potential for metabolic disturbances, cardiovascular adverse effects, and excessive daytime sedation necessitates careful patient selection, individualized benefit–risk assessment, and appropriate long-term monitoring. Overall, quetiapine remains an important therapeutic option for improving sleep when insomnia occurs as part of an underlying psychiatric illness and treatment is guided by evidence-based clinical practice.
REFERENCES

Amit Rathore*, Lalit Verma, Lokesh Kumar, Nitin Saini, K. M. Sweta, The Sleep-Promoting Effects of Quetiapine: A Critical Review of Mechanisms and Clinical Evidence, Int. J. Med. Pharm. Sci., 2026, 2 (7), 672-696. https://doi.org/10.5281/zenodo.21363733
 10.5281/zenodo.21363733
10.5281/zenodo.21363733