
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1School of Health & Allied Sciences, Career Point University, Kota, Rajasthan, India.
2Banaras Hindu University, Varanasi, Uttar Pradesh, India
Objective: The present study was undertaken to evaluate the antiurolithiatic activity of a standardized polyherbal formulation against ethylene glycol-induced urolithiasis in experimental rats. Methods: Hydroalcoholic extracts of selected medicinal plants were prepared by cold percolation method and formulated into a polyherbal formulation. Based on preliminary screening studies, formulation F3 was selected for in-vivo evaluation. Experimental urolithiasis was induced in Wistar albino rats using 0.75% v/v ethylene glycol and 1% w/v ammonium chloride for 28 days. The antiurolithiatic activity of formulation F3 was evaluated at different dose levels by estimating urinary biochemical parameters, serum biochemical markers, renal antioxidant enzymes, and histopathological changes. Acute oral toxicity study was also carried out according to OECD guideline 423. Results: Administration of ethylene glycol significantly increased urinary calcium, oxalate, phosphate, and uric acid levels along with elevated serum creatinine, blood urea, and uric acid levels in urolithiatic rats. Treatment with polyherbal formulation F3 produced significant and dose-dependent reduction in urinary lithogenic constituents and restored altered serum biochemical parameters toward normal values. The formulation also improved renal antioxidant status by increasing SOD, CAT, and GSH levels while reducing MDA levels. Histopathological evaluation demonstrated marked reduction in calcium oxalate crystal deposition and improvement in renal architecture. Among all tested doses, F3 at 600 mg/kg exhibited maximum antiurolithiatic activity comparable with the standard drug-treated group. Conclusion: The findings suggest that the standardized polyherbal formulation possesses significant antiurolithiatic potential and may serve as a promising herbal therapeutic candidate for the prevention and management of urolithiasis.
Urolithiasis is a very common condition of the urinary system in which stones develop in the urinary bladder, ureters or kidneys. It is an extremely painful condition of the urinary system and is a problem that affects millions of people throughout the world 1. Unhealthy dietary habits, sedentary lifestyle, dehydration, metabolic disorders and environmental factors have contributed to an increase in the prevalence of kidney stone disease. Calcium oxalate stones are the most prevalent urinary stones in the body, and make up almost 70–80% of all renal stones 2. The formation of kidney stones is a process that includes the supersaturation of the urine, the initiation of crystals, crystal growth, crystal aggregation and crystal retention in the renal tubules. Urolithiasis is caused by a number of factors including, hyperoxaluria, hypercalciuria, UTI, oxidative stress, and low urine volume. Calcium oxalate crystals may cause damage to the renal epithelial cells and result in abnormal kidney function 3. Ethylene glycol-induced urolithiasis is considered as one of the most commonly adopted experimental models for the evaluation of antiurolithiatic agents. Ethylene glycol is converted into oxalic acid causing hyperoxaluria and calcium oxalate crystals in renal tissues. It is a very similar model to human urolithiasis and is extensively used for pharmacological studies 4. Conventional treatment of urolithiasis may involve use of surgical procedures, lithotripsy and pharmacological treatment 5. But, they can cause recurrence of stones, side effects, stone removal rate is not complete, and the treatment is costly. Thus, there is a growing interest in the use of herbal medicines as alternative and safer treatments in the control of kidney stones due to their low cost 6. Medicinal plants are rich sources of some phytoconstituents possessing antioxidant, diuretic and crystal inhibitory activities like flavonoids, phenolics, terpenoids, tannins, glycosides, and saponins. The multi-medicinal plant containing polyherbal formulations are believed to be more effective since synergistic effect may be achieved with less toxicity 7. Hence, the present study was designed to assess the efficacy of standardized polyherbal formulation on ethylene glycol induced urolithiasis experimental rats. This study aimed at examining how the formulation would impact on urinary parameters, serum biochemical markers, body weight, haematological profile and histopathological changes in calcium oxalate stone formation.
MATERIALS AND METHODS
2.1 Collection and Authentication of Plant Materials
The medicinal plants used in the present investigation were purchased from the local herbal markets as well as from surrounding regions of Uttar Pradesh, India. The plant parts collected were roots, seeds, fruits, leaves, stem bark and whole plants of selected medicinal plants used for urinary disorders and kidney stones. All the plant material collected were identified by Dr. Rajani Srivastava, Assistant Professor (IED), Banaras Hindu University, Mirzapur, UP, India. Voucher specimens were kept in the departmental herbarium. Once authenticated, the plants were washed to get rid of dirt and other foreign particles. The materials were shade dried at room temperature for some days and then coarsely ground with mechanical grinding mill. The drugs were powdered for further experimental studies and stored in airtight containers 8.
2.2 Preparation of Hydroalcoholic Extracts
The dried powdered plant materials were extracted using hydroalcoholic solvent (70:30 ethanol:water) by cold percolation method. The solvents according to the solvent system were added to the accurately weighed powdered drugs and extracted with occasional stirring for 72 h 9. Once the extraction was done, the mixtures were filtered with muslin cloth and Whatman filter paper. Filtrates collected were subjected to reduced pressure using a rotary evaporator and then further dried to get semisolid extracts. The dried extracts were weighed and the percentage yield was calculated and the extracts were kept in air-tight containers for further study 10.
2.3 Preparation of Polyherbal Formulation
The polyherbal formulation was prepared by mixing the dried hydroalcoholic extracts of the selected medicinal plants in certain proportions by the geometric mixing method. The formulated product was then ground to a fine homogeneous powder and kept in airtight containers for subsequent use. Formulation F3 with maximum result on phytochemical screening and in-vitro antiurolithiatic activity was selected for in-vivo antiurolithiatic studies 11.
2.4 Experimental Animals
About 150-200 g healthy adult Wistar albino rats of either gender were used for the present study. Animals were acquired from the institutional animal house facility, and were raised in the standard laboratory conditions with controlled temperature and humidity and a light/dark cycle of 12 h. Throughout the experimental period, all animals were fed pellet diet and water ad libitum 12. The experimental protocol was approved by the Institutional Animal Ethics Committee (IAEC) of United Institute of Pharmacy, Prayagraj, Uttar Pradesh, India following CPCSEA guidelines (CPCSEA No.1451/PO/Re/S/11). The study protocol approval number is UIP/IAEC/Nov. 2025/20 dated 25/11/2025. All experimental procedures on animals were conducted as per guidelines of the Committee for the Purpose of Control and Supervision of Experiments on Animals (CPCSEA), Government of India.
2.5 Acute Oral Toxicity Study
The selected polyherbal formulation (F3) was subjected to the Acute oral toxicity study as per OECD guideline 423, Acute toxic class method. The healthy Wistar albino rats were randomly divided into experimental groups and fasted overnight before giving them the doses with water ad libitum. The polyherbal formulation was orally administered at different doses and the animals were continuously observed for behavioral, neurologic and autonomic changes for the first 4 h after administration. Additional observation occurred every hour for 24 h and daily for 14 days to determine the toxicity or death symptoms 13. All parameters were carefully observed throughout the study period, including body weight, food intake, water intake, skin changes, appearance of fur, changes in mucous membranes, tremors, convulsions, salivation, diarrhea, lethargy, sleep, coma and mortality. Hematological parameters and differential leucocyte count were also determined towards the end of the experimental period to determine the safety profile of the formulation 14.
2.6 Induction of Ethylene Glycol-Induced Urolithiasis
Laboratory induced urolithiasis in Wistar albino rats was effected by ethylene glycol. Hyperoxaluria and calcium oxalate crystal deposition were induced in animals by giving them drinking water containing 0.75% v/v ethylene glycol for 28 days. Ethylene glycol is converted to oxalic acid in the body, which causes oxalate to be present in higher concentrations in the urine and the development of calcium oxalate crystals in the renal tubules. This experimental model is well-adopted and is similar to the human calcium oxalate urolithiasis 15.
2.7 Experimental Design
Animals were randomly divided into six groups containing five animals in each group.
Table 1: Experimental Design for Ethylene Glycol-Induced Urolithiasis Study
|
Group |
Treatment |
|
Group I |
Normal control received vehicle (0.5% CMC, p.o.) once daily for 28 days |
|
Group II |
Urolithiatic control received 0.75% v/v ethylene glycol and 1% w/v ammonium chloride in drinking water for 14 days followed by vehicle treatment |
|
Group III |
Received 0.75% v/v ethylene glycol and 1% w/v ammonium chloride along with standard drug Cystone (750 mg/kg, p.o.). |
|
Group IV |
Received polyherbal formulation F3 (200 mg/kg, p.o.) |
|
Group V |
Received polyherbal formulation F3 (400 mg/kg, p.o.) |
|
Group VI |
Received polyherbal formulation F3 (600 mg/kg, p.o.) |
Hyperoxaluria and calcium oxalate crystal deposition in the renal tissues was induced by ethylene glycol and ammonium chloride respectively. The treatment, with the standard drug and polyherbal formulation, was continued every day for 28 consecutive days. Urine, blood samples and kidney tissue were taken at the end of the experimental period for biochemical analysis in urine, biochemical estimation in serum, antioxidant and histopathology studies 16.
2.8 Collection of Urine and Biochemical Analysis
At the end of the experimental period, animals were individually housed in metabolic cages for 24 h urine collection. The total volume of urine was collected and urine was centrifuged to remove debris and insoluble matter. The clear supernatant obtained was used for biochemical analysis. Standard laboratory tests were performed to assess the degree of lithogenic changes and calcium oxalate crystal formation, and urinary biochemical parameters were estimated, such as calcium, oxalate, phosphate, and uric acid. Improved urine output of these is regarded as one of the important indicator of urolithiasis 17.
2.9 Serum Biochemical Analysis
At the end of treatment period, blood was taken from the retro-orbital puncture under light anesthesia. Serums were collected from the centrifuged blood samples for biochemical estimation. The serum biochemical markers such as serum creatinine, blood urea, uric acid were measured by using standard diagnostic kits. The following parameters were assessed to determine renal functional changes in ethylene glycol induced urolithiasis 18.
2.10 Kidney Antioxidant Parameters
Immediately after sacrifice, kidney tissues were homogenized in ice-cold phosphate buffer solution. Homogenates were centrifuged and the extracts were used for the estimation of antioxidant. To assess the oxidative stress that results from calcium oxalate crystal deposition, the renal antioxidant parameters superoxide dismutase (SOD), catalase (CAT), reduced glutathione (GSH) and lipid peroxidation marker malondialdehyde (MDA) was determined by standard biochemical methods 19.
2.11 Histopathological Evaluation
Experimental animals were sacrificed and kidney tissues were washed in normal saline and fixed in 10% neutral buffered formalin solution. The tissues were processed by routine histological procedures and embedded in paraffin wax. Thin section (5 µm) were prepared, with hematoxylin and eosin (H&E) staining. Stained tissue sections were examined in light microscope to assess renal histopathological changes such as calcium oxalate crystal deposition, tubular dilation, epithelial degeneration, inflammatory infiltration and renal architecture distortion. Representative tissue sections were photographed and these were compared 20.
2.12 Statistical Analysis
All experimental values were expressed as Mean ± SEM. Statistical analysis was performed using one-way analysis of variance (ANOVA) followed by Dunnett’s multiple comparison test. Values of p < 0.05 were considered statistically significant 21.
RESULTS AND DISCUSSION
3.1 Percentage Extractive Yield of Hydroalcoholic Extracts
The extracts produced by the hydroalcoholic extraction of the selected medicinal plants were satisfactory with varying percentage yields of the semisolid extracts. Moringa oleifera, Plectranthus barbatus and Bergenia ligulata have comparatively high extractive yield among all extracts. The percentage of extractive yields in the hydroalcoholic extracts is shown in Table 2.
Table 2: Percentage Extractive Yield of Hydroalcoholic Extracts
|
S. No. |
Plant Name |
Part Used |
Percentage Yield (% w/w) |
|
1 |
Tribulus terrestris |
Fruit |
12.8 ± 0.6 |
|
2 |
Caesalpinia bonducella |
Seed |
10.4 ± 0.5 |
|
3 |
Xanthium strumarium |
Whole plant |
11.2 ± 0.4 |
|
4 |
Phaseolus vulgaris |
Seed |
9.8 ± 0.3 |
|
5 |
Moringa oleifera |
Leaf |
14.6 ± 0.7 |
|
6 |
Bergenia ligulata |
Rhizome |
13.1 ± 0.5 |
|
7 |
Acorus calamus |
Rhizome |
8.9 ± 0.4 |
|
8 |
Desmodium gangeticum |
Root |
10.7 ± 0.5 |
|
9 |
Daucus carota |
Seed |
9.5 ± 0.4 |
|
10 |
Piper cubeba |
Fruit |
11.9 ± 0.6 |
|
11 |
Adiantum capillus-veneris |
Whole plant |
10.1 ± 0.5 |
|
12 |
Chenopodium album |
Leaf |
12.4 ± 0.6 |
|
13 |
Plectranthus barbatus |
Root |
13.8 ± 0.7 |
Values are expressed as Mean ± SEM (n = 3).
3.2 Organoleptic Evaluation of Polyherbal Formulations
The organoleptic property of all developed polyherbal formulations were acceptable with characteristic herbal smell and appearance was uniform. The formulations F3 was more homogeneous, smooth and fine than F1 and F2. Developed formulations are shown in Table 3 and their organoleptic properties are described.
Table 3: Organoleptic Evaluation of Polyherbal Formulations
|
Formulation |
Color |
Odor |
Texture |
Appearance |
|
F1 |
Light brown |
Characteristic herbal |
Slightly coarse |
Non-uniform |
|
F2 |
Brown |
Aromatic herbal |
Fine |
Uniform |
|
F3 |
Dark brown |
Pleasant herbal |
Fine and smooth |
Homogeneous |
3.3 Acute Oral Toxicity Study
The acute oral toxicity study of polyherbal formulation F3 was carried out according to OECD guideline 423. No deaths or apparent signs of toxicity were recorded in any treatment groups in the experiment. Formulation F3 animals remained healthy, active and well throughout the study period. No signs of abnormal behavior including tremors, convulsions, salivation, diarrhea, lethargy or coma were observed. The food, water intake, fur appearance and locomotor activity were not different from controls. There was no toxic effect on growth and metabolic activity of the treated animals, as evident from the normal increase in body weight (Table 4 and Figure 1). Another hematological parameter that was measured in all treated groups was within normal physiological range (Table 5). Also, the presence of differential leucocyte count was within normal physiological range in all treated groups (Table 6). The results indicated that formulation F3 was safe and well tolerated when administered at the given doses.
Table 4: Effect of Polyherbal Formulation on Body Weight During Acute Oral Toxicity Study
|
Group |
Initial Body Weight (g) |
Final Body Weight (g) |
|
Control |
182.4 ± 4.3 |
196.8 ± 5.1 |
|
F3 (200 mg/kg) |
181.7 ± 5.2 |
198.2 ± 4.8 |
|
F3 (400 mg/kg) |
183.5 ± 4.9 |
201.4 ± 5.3 |
|
F3 (600 mg/kg) |
184.1 ± 5.4 |
203.6 ± 5.7 |
Values are expressed as Mean ± SEM (n = 5)
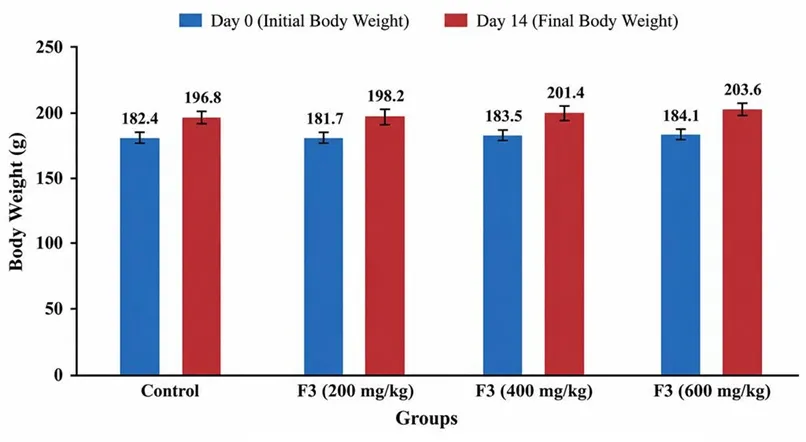
Figure 1: Effect of Polyherbal Formulation on Body Weight During Acute Oral Toxicity Study
Table 5: Effect of Polyherbal Formulation on Hematological Parameters During Acute Oral Toxicity Study
|
Parameter |
Control |
F3 (200 mg/kg) |
F3 (400 mg/kg) |
F3 (600 mg/kg) |
|
Hemoglobin (g/dL) |
13.8 ± 0.4 |
13.9 ± 0.3 |
14.1 ± 0.4 |
14.2 ± 0.5 |
|
RBC (×10⁶/mm³) |
7.1 ± 0.2 |
7.2 ± 0.3 |
7.3 ± 0.2 |
7.4 ± 0.3 |
|
WBC (×10³/mm³) |
8.4 ± 0.4 |
8.2 ± 0.5 |
8.1 ± 0.3 |
8.0 ± 0.4 |
|
Platelets (×10³/mm³) |
640 ± 18 |
648 ± 16 |
652 ± 19 |
658 ± 21 |
Values are expressed as Mean ± SEM (n = 5).
Table 6: Effect of Polyherbal Formulation on Differential Leucocyte Count During Acute Oral Toxicity Study
|
Parameter |
Control |
F3 (200 mg/kg) |
F3 (400 mg/kg) |
F3 (600 mg/kg) |
|
Neutrophils (%) |
28.4 ± 1.2 |
27.9 ± 1.1 |
27.3 ± 1.0 |
26.8 ± 1.2 |
|
Lymphocytes (%) |
64.2 ± 1.5 |
64.8 ± 1.3 |
65.1 ± 1.4 |
65.6 ± 1.2 |
|
Eosinophils (%) |
2.6 ± 0.3 |
2.4 ± 0.2 |
2.3 ± 0.2 |
2.2 ± 0.2 |
|
Monocytes (%) |
3.1 ± 0.2 |
3.0 ± 0.2 |
2.9 ± 0.3 |
2.8 ± 0.2 |
|
Basophils (%) |
1.7 ± 0.1 |
1.9 ± 0.2 |
2.0 ± 0.1 |
2.1 ± 0.2 |
Values are expressed as Mean ± SEM (n = 5).
3.4 Effect of Polyherbal Formulation on Urinary Biochemical Parameters in Ethylene Glycol-Induced Urolithiasis
Significant increases in urinary biochemical parameters were observed after administration of ethylene glycol and ammonium chloride group when compared to normal control group. Higher urinary calcium, oxalate, phosphate and uric acid values were associated with an increased calcium oxalate crystal formation and progression of the urolithiasis. The treatment with polyherbal formulation F3 resulted in significant (p<0.05) reduction in urinary lithogenic parameters in a dose dependent manner in comparison to the disease control group. The level of urinary calcium, oxalate, phosphate and uric acid levels was significantly reduced in the F3 group (600 mg/kg) as compared to all the other treated groups, a result that was similar to the standard drug-treated group. Table 7 and figures 2-5 show the effect of polyherbal formulation to urinary biochemical parameters.
Table 7: Effect of Polyherbal Formulation on Urinary Biochemical Parameters in Ethylene Glycol-Induced Urolithiasis
|
Group |
Calcium (mg/dL) |
Oxalate (mg/dL) |
Phosphate (mg/dL) |
Uric Acid (mg/dL) |
|
Normal Control |
4.8 ± 0.4 |
2.1 ± 0.2 |
3.9 ± 0.3 |
1.8 ± 0.1 |
|
Urolithiatic Control |
11.9 ± 0.9 |
8.6 ± 0.7 |
9.8 ± 0.8 |
5.7 ± 0.4 |
|
Standard (Cystone) |
5.9 ± 0.5*** |
3.0 ± 0.3*** |
4.8 ± 0.4*** |
2.3 ± 0.2*** |
|
F3 (200 mg/kg) |
8.7 ± 0.7* |
5.9 ± 0.5* |
7.2 ± 0.6* |
4.1 ± 0.3* |
|
F3 (400 mg/kg) |
7.1 ± 0.6** |
4.6 ± 0.4** |
6.0 ± 0.5** |
3.3 ± 0.2** |
|
F3 (600 mg/kg) |
6.2 ± 0.5*** |
3.5 ± 0.3*** |
5.1 ± 0.4*** |
2.5 ± 0.2*** |
Values are expressed as Mean ± SEM (n = 5). Statistical significance: *p < 0.05, **p < 0.01, ***p < 0.001 compared with urolithiatic control group.
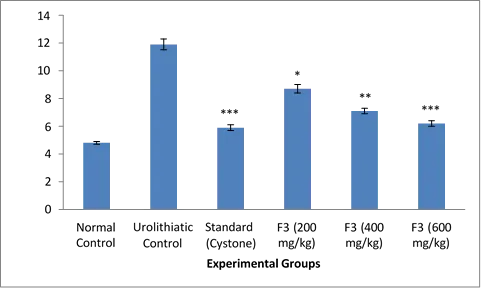
Figure 2: Effect of polyherbal formulation F3 on urinary calcium levels in ethylene glycol-induced urolithiasis.
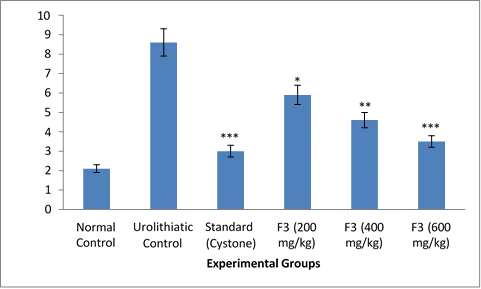
Figure 3: Effect of polyherbal formulation F3 on urinary oxalate levels in ethylene glycol-induced urolithiasis
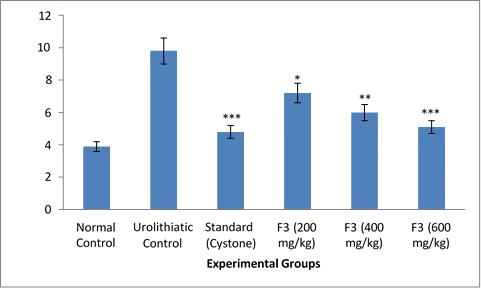
Figure 4: Effect of polyherbal formulation F3 on urinary Phosphate levels in ethylene glycol-induced urolithiasis
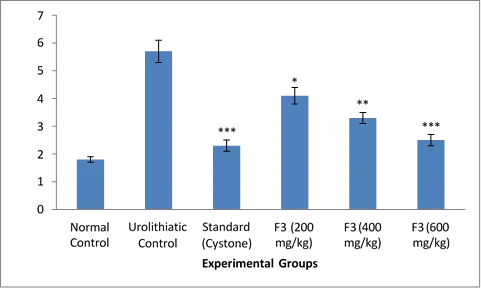
Figure 5: Effect of polyherbal formulation F3 on urinary Uric Acid levels in ethylene glycol-induced urolithiasis
3.5 Effect of Polyherbal Formulation on Serum Biochemical Parameters in Ethylene Glycol-Induced Urolithiasis
In the disease control group, significant difference was observed in the serum biochemical markers between the two groups when compared with the normal control group after administration of ethylene glycol and ammonium chloride. Renal dysfunction was suggested by the raised serum creatinine level, blood urea and uric acid indicating the deposition of calcium oxalate crystals. The use of polyherbal formulation F3 significantly lowered the biochemical parameters of the blood in a dose-dependent manner than the disease control group. The serum creatinine, blood urea and uric acid levels were significantly reduced in all treated groups with maximum reduction observed in F3 group (600 mg/kg) similar to the standard drug treated group. Table 8 and Figures 6-7 shows the effect of polyherbal formulation on serum biochemical parameters.
Table 8: Effect of Polyherbal Formulation on Serum Biochemical Parameters in Ethylene Glycol-Induced Urolithiasis
|
Group |
Serum Creatinine (mg/dL) |
Blood Urea (mg/dL) |
Uric Acid (mg/dL) |
|
Normal Control |
0.72 ± 0.05 |
27.4 ± 1.8 |
1.9 ± 0.2 |
|
Urolithiatic Control |
1.86 ± 0.11 |
58.6 ± 3.4 |
5.9 ± 0.5 |
|
Standard (Cystone) |
0.88 ± 0.07*** |
31.2 ± 2.1*** |
2.4 ± 0.2*** |
|
F3 (200 mg/kg) |
1.42 ± 0.10* |
46.3 ± 2.9* |
4.3 ± 0.4* |
|
F3 (400 mg/kg) |
1.16 ± 0.08** |
39.7 ± 2.5** |
3.5 ± 0.3** |
|
F3 (600 mg/kg) |
0.94 ± 0.07*** |
33.8 ± 2.2*** |
2.7 ± 0.2*** |
Values are expressed as Mean ± SEM (n = 5). Statistical significance: *p < 0.05, **p < 0.01, ***p < 0.001 compared with urolithiatic control group.
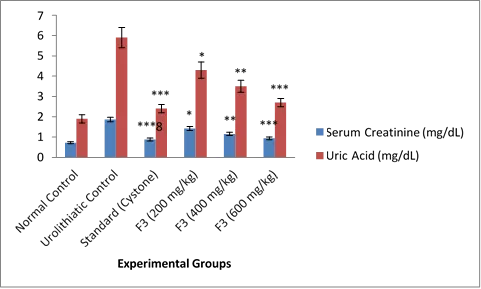
Figure 6: Effect of polyherbal formulation F3 on serum creatinine and uric acid levels in ethylene glycol-induced urolithiasis
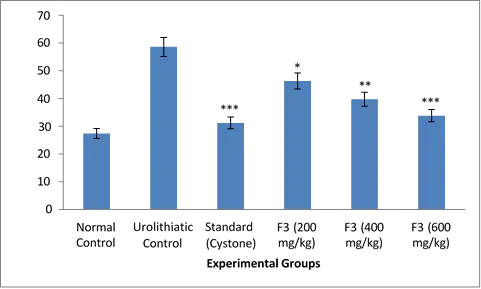
Figure 7: Effect of polyherbal formulation F3 on blood urea levels in ethylene glycol-induced urolithiasis
Effect of Polyherbal Formulation on Kidney Antioxidant Parameters in Ethylene Glycol-Induced Urolithiasis Significant oxidative stress was induced in renal tissues of disease control group after administration of ethylene glycol and ammonium chloride. The disease control group had significant decrease in endogenous antioxidant enzymes such as superoxide dismutase (SOD), catalase (CAT) and reduced glutathione (GSH) and significant increase in malondialdehyde (MDA) levels compared to the normal control group. Renal antioxidant status was restored significantly by treatment with F3 (polyherbal formulation), in a dose dependent manner. The antioxidant enzyme levels were highest in F3 at 600 mg/kg and MDA, the lipid peroxidation marker, was significantly reduced as compared to the standard drug treated group among all treated groups. Table 9 shows the antioxidant parameters of kidneys and Figures 8–9 depict the effect of polyherbal formulation on kidneys antioxidant parameters.
Table 9: Effect of Polyherbal Formulation on Kidney Antioxidant Parameters in Ethylene Glycol-Induced Urolithiasis
|
Group |
MDA (nmol/mg protein) |
SOD (U/mg protein) |
CAT (U/mg protein) |
GSH (µg/mg protein) |
|
Normal Control |
2.4 ± 0.2 |
8.9 ± 0.7 |
42.8 ± 2.5 |
7.6 ± 0.6 |
|
Urolithiatic Control |
7.8 ± 0.6 |
3.2 ± 0.3 |
21.4 ± 1.8 |
3.1 ± 0.3 |
|
Standard (Cystone) |
3.1 ± 0.3*** |
7.9 ± 0.6*** |
39.2 ± 2.2*** |
6.9 ± 0.5*** |
|
F3 (200 mg/kg) |
5.9 ± 0.5* |
4.8 ± 0.4* |
28.7 ± 2.0* |
4.8 ± 0.4* |
|
F3 (400 mg/kg) |
4.6 ± 0.4** |
6.1 ± 0.5** |
33.6 ± 2.1** |
5.9 ± 0.5** |
|
F3 (600 mg/kg) |
3.5 ± 0.3*** |
7.2 ± 0.6*** |
37.4 ± 2.3*** |
6.5 ± 0.4*** |
Values are expressed as Mean ± SEM (n = 5). Statistical significance: *p < 0.05, **p < 0.01, ***p < 0.001 compared with urolithiatic control group.
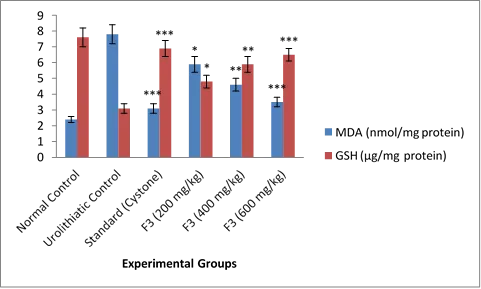
Figure 8: Effect of polyherbal formulation F3 on renal MDA and GSH levels in ethylene glycol-induced urolithiasis.
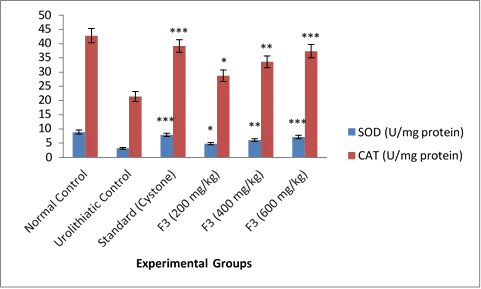
Figure 9: Effect of polyherbal formulation F3 on renal SOD and CAT levels in ethylene glycol-induced urolithiasis.
3.7 Histopathological Evaluation of Kidney Tissue
Histopathological examination of kidney tissues from the normal control group showed normal renal architecture with intact glomeruli and renal tubules without any crystal deposition or inflammatory changes. The urolithiatic control group showed marked histopathological alterations including extensive calcium oxalate crystal deposition, tubular dilation, epithelial degeneration, inflammatory cell infiltration, and distortion of normal renal architecture. Treatment with standard drug Cystone and polyherbal formulation F3 produced significant protection against renal tissue damage. Animals treated with formulation F3 showed reduction in calcium oxalate crystal deposition and improvement in renal histoarchitecture in a dose-dependent manner. Among all treated groups, F3 at 600 mg/kg exhibited maximum protective effect with near-normal renal architecture, minimal crystal deposition, and reduced inflammatory changes compared with the urolithiatic control group. The histopathological observations of kidney tissues are presented in Figure 10.
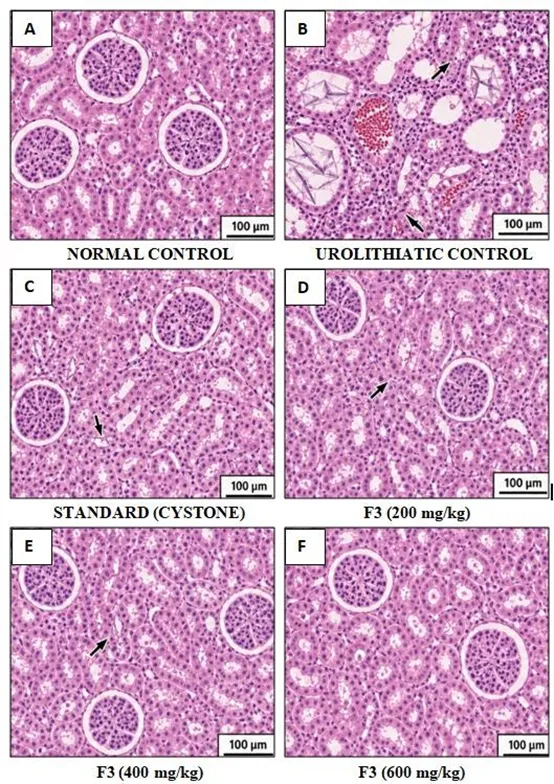
Figure 10: Histopathological Evaluation of Kidney Tissues in Ethylene Glycol-Induced Urolithiasis
DISCUSSION
Urolithiasis is a multifactorial disease that involves the development and accumulation of urinary stones in the urinary system. The most common type of kidney stone is calcium oxalate stone which is strongly linked with hyperoxaluria, oxidative stress, and renal tubular damage. In the present study, ethylene glycol-induced urolithiasis was successfully developed in experimental rats that is similar to calcium oxalate nephrolithiasis in humans. The semisolid extracts obtained from selected medicinal plants by the hydroalcoholic extraction method were good, and the percentage extractive values (PEV) were variable as shown in Table 2. The increase in extractive yield of Moringa oleifera, Plectranthus barbatus and Bergenia ligulata could be due to their presence of polar phytoconstituents like flavonoids, phenolics, glycosides and tannins. The developed polyherbal formulations had acceptable organoleptic property and formulation F3 had a better uniformity and appearance than other formulations (Table 3). Acute oral toxicity evaluation showed that the administration of formulation F3 did not cause toxicity or discomfort at the doses employed. During the study period there were no deaths or indications of toxicity. Normal weight gain was observed in all treated groups which was confirmed by body weight analysis, and it was found that there was no toxic effect of the treatments on the normal physiological functions (Table 4 and Figure 1). Likewise, the hematological parameters and the differential leucocyte count were in normal physiological levels confirming the safety of the formulation (Table 5 and 6). Ethylene glycol and ammonium chloride administration resulted in significant increase in urinary calcium, oxalate, phosphate and uric acid concentration in the urolithiatic control group. Urine is made more supersaturated with these lithogenic constituents, thus favoring the nucleation, aggregation and retention of calcium oxalate crystals in renal tubules. Treatment with polyherbal formulation F3 significantly lowered the urinary biochemical parameters in a dose dependent fashion (Table 7 and Figures 2-5). F3 at 600 mg/kg had the greatest inhibitory effect on the urinary lithogenic markers, indicating its most powerful inhibition of calcium oxalate crystal formation among all treated groups. The urolithiatic control group showed significant increase in serum creatinine, blood urea and uric acid levels which pointed towards renal dysfunction due to crystal deposition and tubular damage. Acute renal failure is defined by an increase in serum creatinine and in blood urea concentration. The biochemical parameters were effectively reversed to normal levels with dose dependent effects of formulation F3 (Table 8 and Figures 6–7). This may be related to the protective effects on renal function and reduction in crystal burden and maintenance of integrity of renal tubules seen with the formulation. Oxidative stress is an important factor in calcium oxalate-induced renal epithelial injury and crystal retention. The present study revealed that administration of ethylene glycol significantly reduced the activity of endogenous antioxidant enzymes such as SOD, CAT and GSH and enhanced lipid peroxidation marker MDA in renal tissues. Decreased antioxidant defenses lead to damage of the cell membrane and to renal inflammation and crystal adhesion. However, administration of polyherbal formulation F3 significantly enhanced the level of antioxidant enzymes in the kidney and decreased the concentration of MDA, suggesting that it was able to attenuate oxidative stress and lipid peroxidation (Table 9 and figures 8–9). The anti-oxidant activity of the formulation could be due to the flavonoids, phenolics and terpenoids that are present in the selected medicinal plants. The histopathological examination also confirmed the biochemical results. The kidney tissues of the normal control group had intact glomeruli and normal renal architecture while in the urolithiatic control group extensive calcium oxalate crystal deposits, tubular dilation, epithelial degeneration and inflammatory infiltrations were seen. Significant improvement was observed in renal histoarchitecture in both the standard drug Cystone and formulation F3 with reduction in renal crystal deposits and inflammatory changes (Figure 10). F3 (600 mg/kg) exhibited near-normal renal architecture and provided maximum protection against renal tissue injury among all treated groups. The developed polyherbal formula has shown a significant antiurolithiatic effect which could be due to the synergistic effect of various bioactive phytoconstituents in the selected medicinal plants. The phytoconstituents of these plants are known for their antioxidant, anti-inflammatory, diuretic and crystal inhibitory effects that all play a role in preventing calcium oxalate stone formation and damage to the kidneys. The results obtained from present investigation indicate that standardized polyherbal formulation has substantial protection against ethylene glycol induced urolithiasis and can be considered as a potential herbal therapeutic agent for the treatment of kidney stone disease.
CONCLUSION
In the present investigation, it has been shown that the standardized polyherbal formulation has significant anti urolithiasis activity in ethylene glycol induced urolithiasis experimental rats. Hyperoxaluria, calcium oxalate crystal deposition, oxidative stress and renal dysfunction were successfully induced in this study using ethylene glycol and ammonium chloride that closely mimics human urolithiasis. The urinary lithogenic constituents like calcium, oxalate, phosphate and uric acid was found to be significantly reduced with the treatment of polyherbal formulation F3. The formulation also normalized the altered serum biochemical parameters and the antioxidant status of the kidney by elevating the level of antioxidant enzymes – SOD, CAT and GSH and decreasing the lipid peroxidation marker – MDA. The formulation was also found to have a protective effect by the histopathological evaluation, which showed a significant decrease in the deposition of calcium oxalate crystals and restoration of normal renal architecture. The antiurolithiatic activity of F3 (600 mg/kg) was found to be the highest among all other tested doses and was similar to the standard drug treated group. The therapeutic effect observed could be due to the synergistic effect of bioactive phytoconstituents found in the medicinal plants selected, including flavonoids, phenolics, tannins, terpenoids and saponins. In general, the results indicate that the preparation of polyherbal formulation developed in this study could be a potential herbal therapeutic agent in the prevention and management of urolithiasis. But more pharmacologic and clinical research is needed to confirm its safety and therapeutic effectiveness over the long term.
ACKNOWLEDGEMENT:
The authors are sincerely thankful to the School of Health & Allied Sciences, Career Point University, Kota, Rajasthan, India, for providing the necessary facilities and support to carry out the present research work.
Conflict of Interest:
The authors declare that there is no conflict of interest regarding the publication of this research work.
REFERENCES

Naresh Kumar Sachan*, Mahesh Gupta, Manju Makhija, Sunil Kumar Singh, Evaluation of a Standardized Polyherbal Formulation Against Ethylene Glycol-Induced Urolithiasis in Rats, Int. J. Med. Pharm. Sci., 2026, 2 (6), 298-311. https://doi.org/10.5281/zenodo.20759920
 10.5281/zenodo.20759920
10.5281/zenodo.20759920