
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Pallavan Pharmacy College, Kanchipuram-631 502
mRNA vaccines, in vitro transcribed since 1961, enable rapid, safe therapies for infectious diseases, immunotherapies, and more surpassing traditional vaccines' limits against HIV, malaria, and mutating influenza. Scalable cell-free production yields millions of multi-antigen doses without mutagenesis risks. Routes like IM/ID optimize efficacy via antigen-presenting cells activating T/B responses. Advances in influenza, rabies, and combos target respiratory threats. Liquid LNPs need −60°C storage, but lyophilization allows 6 months at 4°C. COVID-19 success highlights mRNA's speed and versatility for pandemics.
Messenger RNA (mRNA), identified in 1961 as a transient bridge between DNA and proteins, can now be transcribed in vitro and serves as a promising platform for therapies including immunotherapies, viral vaccines, genome editing, and cellular reprogramming [1]. Vaccination remains the most powerful method for managing infectious diseases, having wiped out smallpox and nearly eradicated polio [2]. The World Health Organization states that vaccines avert 2–3 million deaths each year from illnesses like tetanus, pertussis, influenza, and measles [3,4]. Traditional vaccines struggle against elusive pathogens such as Plasmodium falciparum, hepatitis C, and HIV, which dodge immune detection, and often require frequent reformulation to counter evolving viruses like influenza [5]. Over the past three decades, mRNA vaccines have emerged as safe, adaptable, and straightforward to manufacture, offering key benefits beyond conventional vaccines without concerns over insertional mutagenesis [6]. Its swift, economical cell-free production enables a single liter bioreactor run to yield almost one million doses. Plus, one mRNA vaccine can encode several antigens at once, boosting immunity to multiple pathogens. Once doubted for stability, efficacy, and excessive immune activation, mRNA technology has gained fresh momentum in clinical use over the last decade, thanks to progress in pharmacology, delivery systems, and immunogenicity control [7].
Route of Administration Of mRNA
The administration route of mRNA vaccines greatly influences their effectiveness. Common injection methods include intradermal (ID), subcutaneous (SC), intramuscular (IM), intranasal (IN), and intravenous (IV). Other routes, such as intranasal, intravaginal, and intratumoral injections, have also been investigated. The characteristics of the vaccination site be it skin, muscle, or lymphoid organs affect both safety and efficacy, as vaccines can be delivered through systemic or local methods [8].
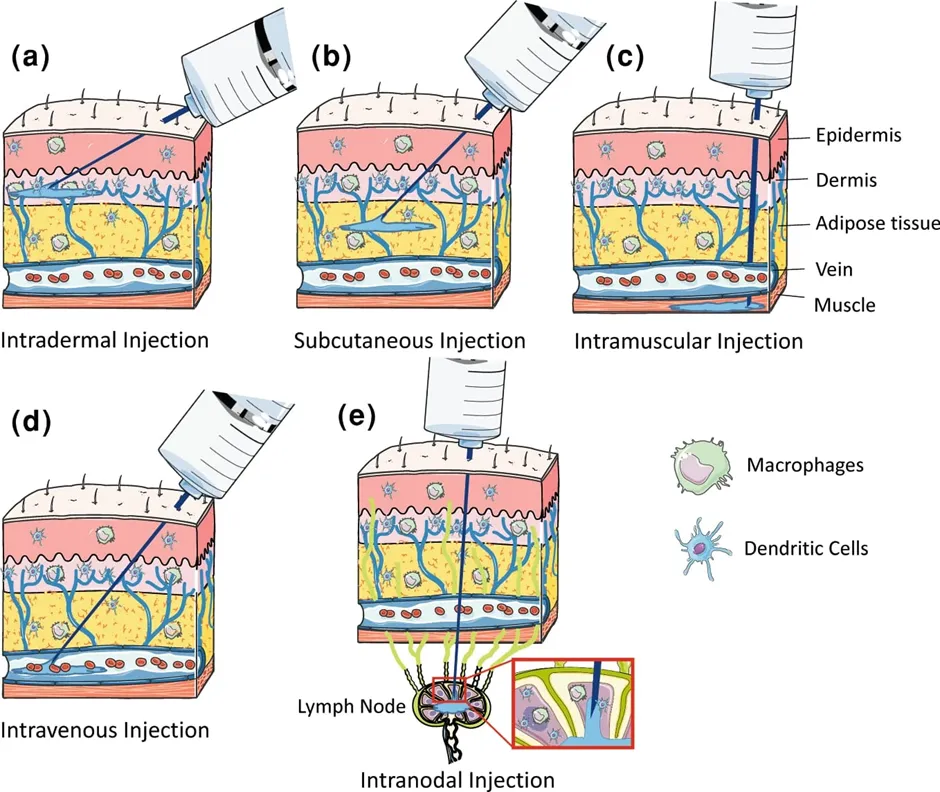
Figure .1. Route of Administration Of mRNA
Progress With mRNA Vaccine for Infectious Disease mRNA
Recent advancements in therapeutics have led to significant progress in vaccine development for infectious diseases. Currently, most mRNA vaccines, undergoing preclinical and clinical testing, are administered through bolus injection into the skin, muscle, or subcutaneous tissue. This method facilitates mRNA uptake by immunological and non-immunological cells, enabling the translation into antigens that activate T and B cells. Both mRNA and its delivery mechanisms are vital for improving the immunogenicity and effectiveness of these vaccines [9]. Injected mRNA vaccines are taken up by antigen-presenting cells through endocytosis. Once the mRNA escapes into the cytosol, ribosomes translate it into proteins that activate the immune response. Intracellular antigens are cleaved into smaller fragments by the proteasome and presented on the cell surface to cytotoxic T cells via major histocompatibility complex (MHC) class I proteins [10]. Activated cytotoxic T cells eliminate infected cells by releasing cytolytic molecules such as perforin and granzyme. Furthermore, secreted antigens can be internalized, processed in endosomes, and presented to helper T cells through MHC class II proteins. Helper T cells facilitate the elimination of pathogens by stimulating B cells to produce neutralizing antibodies and activating phagocytes like macrophages via inflammatory cytokines [11].
Influenza Virus mRNA Vaccine
The advent of novel influenza strains highlights the urgent need for vaccinations with accurate antigen design and rapid scalable manufacture. Fortunately, mRNA vaccines with these critical characteristics represent a viable approach for effectively combating rising threats from influenza and other diseases. Before the commencement of the COVID-19 pandemic, substantial efforts were made to designing mRNA vaccines for influenza. These vaccines have been exposed to both preclinical and clinical trials [12].
Rabies Virus mRNA Vaccine
The preventive mRNA vaccine CV7201 (NCT02241135), which was developed using the cationic protein protamine and encoded the rabies virus glycoprotein, was evaluated in a phase 1 trial in 2017. Intradermal and intramuscular administration techniques employing either needle-syringe or needle-free devices were used, along with a variety of dosages and regimens. Although CV7201 was generally tolerable, the mode of administration was necessary to generate adequate immunological responses [13].
Combination mRNA Vaccine
In order to effectively fight acute viral respiratory illnesses with a single injection while simultaneously boosting coverage rates, it is highly desirable to investigate the possibility of combinatorial mRNA vaccines. Combination vaccinations have the potential to improve health outcomes at lower costs due to factors like better uptake, more compliance, lower vaccine administration costs, and improved customer convenience. In the meantime, mRNA vaccines show that they can incorporate different [14].
Storage
The approved mRNA vaccines mRNA-1273 and BNT162b2, both delivered in LNPs, remain viable for 6 months frozen at −20°C and −80 to −60°C, respectively [15]. Once thawed, they stay stable at 2–8°C for up to 1 month. These demanding storage needs complicate worldwide vaccine distribution, prompting numerous studies to tackle the problem. Lyophilized mRNA-LNPs, meanwhile, enable stable storage for 6 months at 4°C and 3 months at room temperature [16,17].
Stability
mRNA is highly vulnerable to RNase enzymes, which readily degrade it. Thus, it demands rigorously sterile, RNase-free conditions during preparation, storage, and administration. All equipment for these stages must be sterile. Yet, against common misconceptions, RNA shows substantial thermodynamic stability in vitro [18]. RNA proves more thermostable but more prone to oxidation than DNA. It stands as the sole biological molecule that withstands heating (up to 90 °C), freezing, lyophilization, precipitation, or resuspension in aqueous media without harm. In general, lyophilized biological products offer superior stability over their liquid counterparts. The lyophilized powder can be reconstituted prior to injection or applied directly for inhalation or intranasal vaccination, provided it exhibits strong aerosol performance [19,20].
CONCLUSION
In conclusion, the demonstrated efficacy of mRNA vaccines against COVID-19 is a significant advancement in vaccine development that highlights persistent issues with conventional technologies, such as scalability, adaptability, and development speed. Because of its adaptability and versatility, mRNA technology is a key weapon in the global fight against endemic diseases and pandemics. Clinical experiments have demonstrated the safety and effectiveness of mRNA vaccines for COVID-19, and mass vaccination has proven beneficial.
ACKNOWLEDGMENT
I would like to thank my guide and faculty for their support in completing this article. I also thank my institution, family, and friends for their encouragement.
REFERENCES


Sasikala E.*, Malarvizhi K., mRNA Vaccines for Infectious Diseases Advances in Design, Delivery, Immunogenicity and Future Perspectives, Int. J. Med. Pharm. Sci., 2026, 2 (7), 409-412. https://doi.org/10.5281/zenodo.21264319
 10.5281/zenodo.21264319
10.5281/zenodo.21264319