
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1Pharm D Intern, Ezhuthachan College of Pharmaceutical Sciences, Marayamuttom Neyyattinkara, Thiruvananthapuram.
2Assistant Professor, Department of Pharmacy Practice, Ezhuthachan College of Pharmaceutical Sciences, Marayamuttom, Neyyattinkara, Thiruvananthapuram.
3Consultant Neurologist, NIMS Medicity, Thiruvananthapuram.
4HOD/Principal, Department of Pharmacy Practice, Ezhuthachan College of Pharmaceutical Sciences, Marayamuttom, Neyyattinkara, Thiruvananthapuram
Paraneoplastic cerebellar degeneration (PCD) is a rare immune-mediated neurological syndrome most commonly associated with breast malignancies and anti-Yo antibodies. It typically presents as subacute cerebellar dysfunction due to autoimmune injury to Purkinje cells. A case of a 72-year-old female with metastatic breast carcinoma who presented with acute onset gait instability, incoordination, dysarthria, progressive breathlessness, and altered sensorium. Neurological examination was suggestive of cerebellar dysfunction with associated encephalopathy. MRI of the brain revealed atypical pontine and temporal lobe changes without evidence of cerebellar atrophy. Paraneoplastic evaluation showed Anti-Yo (PCA-1) antibody positivity. The patient experienced rapid clinical deterioration and succumbed to respiratory failure within six days of hospitalization. This case highlights the importance of considering PCD in patients with malignancy presenting with cerebellar symptoms, even in the presence of atypical imaging findings and concurrent systemic illness.
Paraneoplastic neurological syndromes (PNS) are a heterogeneous group of rare neurological disorders that occur as remote effects of systemic malignancies. These syndromes are not caused by direct tumour invasion, metastasis, infection, or treatment-related complications, but rather by immune-mediated mechanisms triggered by an underlying cancer. Although uncommon, PNS can affect various regions of the nervous system and may significantly contribute to morbidity and mortality in affected patients. (1) Paraneoplastic cerebellar degeneration (PCD) is one of the classical and best-characterized paraneoplastic neurological syndromes. It is most frequently associated with breast and gynaecological malignancies, although it has also been reported in association with other solid tumours. The condition is characterized by rapidly progressive cerebellar dysfunction resulting in symptoms such as gait ataxia, limb incoordination, dysarthria, nystagmus, and postural instability. (2) The pathogenesis of PCD involves an autoimmune response directed against neuronal antigens that are aberrantly expressed by tumour cells. In susceptible individuals, the immune system generates antibodies and cytotoxic T-cell responses against these shared antigens, leading to selective injury of cerebellar Purkinje cells. The resulting neuronal damage is often irreversible and may progress despite treatment, contributing to poor neurological outcomes. (7)
Anti-Yo antibody (PCA-1) is a well-recognized marker of paraneoplastic cerebellar degeneration and is frequently identified in women who have underlying breast cancer. Detection of Anti-Yo antibodies strongly supports the diagnosis in the appropriate clinical setting and has important diagnostic and prognostic implications. However, neurological manifestations may precede or accompany the diagnosis of malignancy, making recognition of the syndrome particularly challenging. (8) The diagnosis of PCD often requires a high index of clinical suspicion because neuroimaging findings may be normal or nonspecific during the early stages of the disease. Furthermore, in patients with advanced malignancy, metabolic disturbances, hypoxia, infection, and structural neurological abnormalities can obscure the clinical picture and delay diagnosis. Therefore, comprehensive clinical evaluation combined with paraneoplastic antibody testing plays a crucial role in establishing the diagnosis and guiding further management. (5) Here we report a case of Anti-Yo–associated paraneoplastic cerebellar degeneration in a 72-year-old female with metastatic breast carcinoma who presented with rapidly progressive cerebellar dysfunction and encephalopathy. This case highlights the diagnostic challenges associated with PCD, particularly in the presence of atypical neuroimaging findings and advanced systemic disease.
CASE PRESENTATION
A 72-year-old female, a known case of metastatic breast carcinoma with lung metastasis and recurrent malignant pleural effusion on palliative care, presented with acute onset unsteadiness of gait, incoordination, and slurred speech. These symptoms were accompanied by progressively worsening breathlessness and reduced responsiveness. On neurological examination, the patient was drowsy but arousable. She had dysarthria and gaze-evoked nystagmus. Bilateral limb ataxia was noted, and her gait was broad-based in the early stage. There was no focal motor weakness. The overall clinical picture was suggestive of cerebellar syndrome with associated encephalopathy.
Laboratory Investigations
These findings indicate isolated protein elevation without pleocytosis, suggestive of a non-inflammatory process.
Neuroimaging
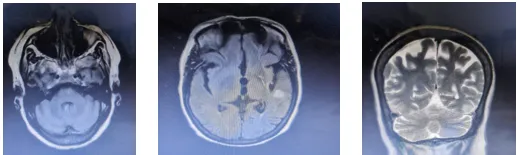
Figure1: MRI BRAIN
MRI brain (non-contrast) revealed features of small vessel disease, along with subtle hyperintensity in the left pons and patchy hyperintensity in the left temporal lobe. No definite cerebellar atrophy was noted.
Paraneoplastic Workup
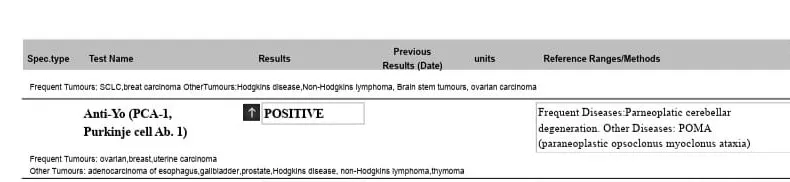
Figure 2: Paraneoplastic neuronal antibody panel showing Anti-Yo (PCA-1) positivity
CLINICAL COURSE
During hospitalization, the patient’s condition deteriorated with worsening breathlessness due to malignant pleural effusion. Her sensorium progressively declined, and she developed respiratory failure. Despite supportive management, she succumbed on the sixth day of admission.
DISCUSSION
Paraneoplastic cerebellar degeneration (PCD) is a rare neurological syndrome associated with underlying malignancies, particularly breast and gynaecological cancers. It results from an immune-mediated response in which antibodies and immune cells directed against tumour antigens also react against cerebellar tissue, especially Purkinje cells. The resulting neuronal damage is often irreversible and may lead to significant neurological disability despite treatment. (7) In the present case, the patient presented with gait instability, slurred speech, limb incoordination, and gaze-evoked nystagmus, which were suggestive of cerebellar dysfunction. Given the history of metastatic breast carcinoma, a paraneoplastic neurological syndrome was considered. The detection of Anti-Yo antibodies further supported the diagnosis and explained the progressive neurological deterioration. The diagnosis was challenging because neurological symptoms in patients with advanced malignancy can occur due to several causes, including metastatic disease, metabolic abnormalities, infections, medication-related adverse effects, and cerebrovascular events. The coexistence of advanced cancer and multiple systemic complications further complicated the clinical picture and made early diagnosis difficult. An important finding in this case was the neuroimaging appearance. Despite significant cerebellar symptoms, MRI did not show definite cerebellar atrophy. Instead, subtle abnormalities were identified in the pons and temporal lobe. Such atypical findings may lead to diagnostic uncertainty and emphasize the importance of correlating imaging findings with clinical and laboratory features rather than relying on radiological findings alone. Cerebrospinal fluid analysis showed elevated protein levels without significant pleocytosis. Although these findings were non-specific, they supported the possibility of a non-infectious neurological process. When interpreted together with the clinical presentation, underlying malignancy, and Anti-Yo antibody positivity, they contributed to the overall diagnostic assessment. Another notable feature of this case was the rapid progression of both neurological and systemic symptoms. During hospitalization, the patient developed worsening respiratory distress secondary to recurrent malignant pleural effusion along with progressive neurological decline. Despite supportive treatment, respiratory failure developed and resulted in death within a few days of admission. Peterson et al. reported that patients with Anti-Yo–associated paraneoplastic cerebellar degeneration commonly present with rapidly progressive cerebellar symptoms such as gait ataxia, dysarthria, and limb incoordination, which were also observed in the present case. Shams’ili et al. noted that cerebellar atrophy is a common neuroimaging finding as the disease progresses. However, unlike their findings, MRI in the present case did not show definite cerebellar atrophy and instead revealed subtle hyperintensities in the pons and temporal lobe. Rojas et al. also reported poor neurological outcomes in patients with Anti-Yo positivity, which is consistent with the rapid neurological deterioration and fatal outcome observed in the present case. Similarly, Graus and Dalmau emphasized the strong association between Anti-Yo antibodies and breast malignancies, which is in agreement with the patient's underlying metastatic breast carcinoma. These similarities and differences demonstrate that Anti-Yo–associated paraneoplastic cerebellar degeneration can present with variable clinical and radiological features, making early recognition essential even when the imaging findings are unusual.
Management of Anti-Yo–associated PCD remains difficult. Various immunomodulatory therapies have been used in an attempt to slow disease progression; however, their effectiveness is often limited once significant neuronal damage has occurred. Early recognition of the syndrome and treatment of the underlying malignancy are considered important factors that may influence outcome. Nevertheless, treatment options are often limited in patients with advanced cancer and multiple coexisting complications. This case highlights the challenges involved in diagnosing paraneoplastic neurological syndromes in patients with advanced malignancy. Multiple possible causes for the neurological symptoms had to be considered before a paraneoplastic cause was identified. The case also demonstrates how rapidly neurological deterioration can occur in Anti-Yo–associated PCD, particularly in the presence of advanced cancer. Careful evaluation of new neurological symptoms in patients with malignancy may help facilitate earlier diagnosis and appropriate management of similar cases.
CONCLUSION
Paraneoplastic cerebellar degeneration is a rare but serious neurological complication of malignancy that can lead to rapid neurological deterioration and significant diagnostic difficulties. This case illustrates how Anti-Yo–associated PCD may present with classical cerebellar symptoms despite atypical neuroimaging findings and multiple coexisting systemic complications. From a clinical perspective, this report highlights the importance of maintaining a high index of suspicion when patients with underlying malignancies develop unexplained neurological symptoms such as gait instability, dysarthria, or incoordination. Early recognition and timely paraneoplastic evaluation may help reduce diagnostic delays and support appropriate management decisions. This case emphasizes that rare neurological complications can sometimes be overlooked in patients with advanced malignancy because clinical attention is often focused on the primary cancer and its associated complications. The appearance of unexplained symptoms such as gait instability, dysarthria, or incoordination should prompt consideration of paraneoplastic neurological syndromes and appropriate diagnostic evaluation. Although Anti-Yo–associated paraneoplastic cerebellar degeneration remains difficult to treat and is often associated with poor outcomes, greater awareness among healthcare professionals and earlier recognition may help support timely management and improve patient care in future cases. Looking ahead, further studies may help clarify the complex mechanisms underlying Anti-Yo–associated paraneoplastic cerebellar degeneration and contribute to the development of earlier diagnostic tools and more effective treatment options.
REFERENCES


Nandana R. S.*, Grace N. Raju, Vipin Venugopalan, Shaiju S. Dharan, Anti-Yo–Associated Paraneoplastic Cerebellar Degeneration in Metastatic Breast Cancer with Rapid Neurological Decline: A Case Report, Int. J. Med. Pharm. Sci., 2026, 2 (7), 436-440. https://doi.org/10.5281/zenodo.21272698
 10.5281/zenodo.21272698
10.5281/zenodo.21272698