
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1Department of Community medicine, BLDE (DU), Shri B.M Patil Medical College Hospital and Research Centre, Vijayapura, Karnataka, India
2Department of Ophthalmology, Hi-Tech Medical College and Hospital, Rourkela, Odisha, India
3Department of Community medicine, Rajarajeshwari Medical College and Hospital, Bengaluru, Karnataka, India
4Department of Community medicine, Bharati Vidyapeeth (deemed to be University) Medical College and hospital, Sangli, Maharashtra, India
Background: Accredited Social Health Activists (ASHAs) play a pivotal role in delivering community-based non-communicable disease (NCD) prevention and health promotion services under India's National Programme for Prevention and Control of Non-Communicable Diseases (NP-NCD). Understanding their experiences is essential for identifying implementation barriers and informing strategies to strengthen primary healthcare services. Aim: To explore the experiences of ASHAs in implementing community-based NCD prevention and health promotion programmes in a rural setting. Methods: A qualitative descriptive study was conducted among 20 ASHAs working in the rural field practice area of a tertiary care teaching institution in Karnataka, India. Participants were selected using purposive sampling. Data were collected through semi-structured in-depth interviews using a pre-tested interview guide. Data saturation was achieved after the 18th interview; however, two additional interviews were conducted to confirm saturation, yielding a final sample of 20 participants. Interviews were audio-recorded, transcribed verbatim, and analysed using Braun and Clarke's reflexive thematic analysis. The study adhered to the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines. Results: Five major themes emerged from the analysis: (a) understanding of NCD prevention, (b) expanding roles and responsibilities of ASHAs, (c) barriers to programme implementation, (d) facilitators and sources of motivation, and (e) recommendations for strengthening community-based NCD prevention. Participants demonstrated good awareness of NCD prevention and acknowledged their expanding role in screening, health education, and referral services. However, increased workload, inadequate logistics, digital reporting challenges, irregular incentives, and limited community participation hindered effective programme implementation. Community trust, supportive supervision, and intrinsic motivation facilitated service delivery. Participants recommended regular refresher training, timely incentives, uninterrupted availability of screening equipment, simplified digital reporting systems, and greater community awareness to enhance programme effectiveness. Conclusion: ASHAs are central to the successful implementation of community-based NCD prevention programmes but face several operational and systemic challenges. Strengthening capacity building, supportive supervision, logistical support, digital infrastructure, and incentive mechanisms may enhance their effectiveness and improve the delivery of primary healthcare services for NCD prevention.
Non-communicable diseases (NCDs), including cardiovascular diseases, diabetes mellitus, chronic respiratory diseases, and cancers, are the leading causes of morbidity and mortality globally. According to the World Health Organization (WHO), NCDs account for approximately 43 million deaths annually, representing nearly 74% of all global deaths. More than three-quarters of these deaths occur in low- and middle-income countries, where health systems face considerable challenges in addressing the growing burden of chronic diseases. Most NCDs are driven by modifiable behavioural risk factors such as tobacco use, unhealthy diets, physical inactivity, and harmful use of alcohol, making prevention and health promotion fundamental components of disease control [1]. India is undergoing a rapid epidemiological transition characterized by a shift from communicable diseases to chronic non-communicable diseases. Currently, NCDs contribute to nearly two-thirds of all deaths in the country and account for a substantial proportion of disability-adjusted life years (DALYs). Population ageing, urbanization, nutritional transition, sedentary lifestyles, and increasing prevalence of obesity have accelerated the burden of hypertension, diabetes, cardiovascular diseases, and common cancers. This escalating burden poses significant challenges to the healthcare system and threatens the achievement of national and global health targets [2–4]. Recognizing the growing burden of NCDs, the Government of India launched the National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases and Stroke (NPCDCS) in 2010, which has subsequently been expanded into the National Programme for Prevention and Control of Non-Communicable Diseases (NP-NCD). The programme is integrated with Comprehensive Primary Health Care under the Ayushman Bharat Health and Wellness Centre initiative and emphasizes health promotion, behaviour change communication, population-based screening of adults aged 30 years and above, early diagnosis, treatment, referral, and long-term follow-up. Effective implementation of these services relies heavily on the primary healthcare system and community-based health workers [5,6]. Accredited Social Health Activists (ASHAs) are the cornerstone of India's community health workforce and serve as a vital link between rural communities and the public health system. Initially introduced under the National Rural Health Mission to improve maternal and child health outcomes, the scope of ASHAs has expanded considerably in recent years. They are now responsible for mobilizing communities for population-based NCD screening, conducting household visits, promoting healthy lifestyle behaviours, identifying individuals at risk, facilitating referrals, ensuring treatment adherence, and providing follow-up support. Their close relationship with the community positions them uniquely to influence health-seeking behaviour and facilitate the prevention and early detection of NCDs [5,7,8]. Despite their expanding responsibilities, ASHAs encounter numerous challenges while implementing NCD-related activities. Increasing workload, competing programme priorities, inadequate training, shortages of logistics and screening equipment, digital reporting requirements, irregular incentives, and varying levels of community awareness may hinder effective programme implementation. These operational constraints can affect the quality and sustainability of community-based NCD prevention services and limit the effectiveness of population-based screening initiatives [8–10]. While several quantitative studies have assessed programme coverage, screening rates, and health outcomes under the NP-NCD programme, they provide limited insight into the contextual factors influencing programme implementation at the grassroots level. Qualitative research offers an opportunity to understand the lived experiences, perceptions, challenges, motivations, and support needs of frontline health workers. Exploring the experiences of ASHAs can generate valuable evidence to strengthen programme implementation, improve training and supportive supervision, enhance community engagement, and inform policy decisions aimed at improving primary healthcare delivery for NCD prevention [9–12]. Although qualitative studies on community health workers have increased in recent years, evidence specifically exploring ASHAs' experiences in implementing community-based NCD prevention and health promotion programmes in rural India remains limited. Understanding their perspectives is essential for identifying implementation barriers and facilitators, optimizing programme delivery, and strengthening community-based strategies for achieving the Sustainable Development Goal target of reducing premature mortality from NCDs by one-third by 2030 [1,6,12]. Therefore, the present study aims to explore the experiences of Accredited Social Health Activists (ASHAs) in implementing community-based non-communicable disease prevention and health promotion programmes in rural India.
MATERIALS AND METHODS
Study Design
A qualitative descriptive study adopting an interpretive approach was conducted to explore the experiences of Accredited Social Health Activists (ASHAs) in implementing community-based non-communicable disease (NCD) prevention and health promotion programmes. The study employed in-depth interviews (IDIs) to gain a comprehensive understanding of the participants' perceptions, experiences, challenges, and recommendations regarding the implementation of NCD-related activities at the community level. The qualitative descriptive design was chosen because it facilitates an in-depth exploration of participants' experiences in their natural settings while providing rich contextual information relevant to programme implementation.
Study Setting
The study was conducted in the rural field practice area attached to the Department of Community Medicine, Vijayapura, Karnataka, India. The study area comprised villages served by Primary Health Centres (PHCs), Health and Wellness Centres (HWCs), and their affiliated sub-centres. Accredited Social Health Activists (ASHAs) working in these villages were actively involved in implementing the National Programme for Prevention and Control of Non-Communicable Diseases (NP-NCD), including community mobilization, population-based screening for hypertension, diabetes, and common cancers, health education, follow-up of diagnosed individuals, referral services, and promotion of healthy lifestyle practices.
Sampling Technique
Participants were selected using a purposive sampling technique to ensure the inclusion of ASHAs with direct experience in implementing community-based NCD prevention activities. ASHAs who had completed at least two years of service and had actively participated in NP-NCD activities were considered eligible for the study. Those who were on prolonged leave during the data collection period or were unwilling to participate were excluded from the study. Participant recruitment continued until data saturation was achieved, defined as the stage at which no new themes or meaningful information emerged from subsequent interviews. A total of 20 Accredited Social Health Activists (ASHAs) participated in the study. Data saturation was achieved after the 18th interview; however, two additional interviews were conducted to confirm that no new themes emerged, resulting in a final sample of 20 participants.
Data Collection
Data were collected from November 2025 to April 2026 through face-to-face semi-structured in-depth interviews using an interview guide developed after an extensive review of the literature and consultation with experts in Community Medicine and qualitative research. The interview guide comprised broad open-ended questions designed to explore participants' perceptions of their roles in NCD prevention, experiences in conducting community-based screening and health promotion activities, challenges encountered during programme implementation, factors facilitating service delivery, and suggestions for improving NCD prevention services. The interview guide was pilot tested among two ASHAs working outside the study area to assess the clarity, relevance, and sequencing of questions. Minor modifications were made based on their feedback, and the pilot interviews were not included in the final analysis. Interviews were conducted by the principal investigator in the participants' preferred language (Kannada, Hindi, or English) at locations convenient to the participants while ensuring privacy and minimal interruption. Prior to each interview, written informed consent was obtained, and permission for audio recording was sought. Each interview lasted approximately 40-60 minutes. Detailed field notes documenting non-verbal expressions, contextual observations, and interviewer reflections were maintained immediately after each interview to supplement the interview transcripts. All audio recordings were transcribed verbatim shortly after data collection. Interviews conducted in Kannada or Hindi were translated into English by bilingual researchers experienced in qualitative research. The translated transcripts were independently reviewed against the original recordings to ensure linguistic accuracy and preservation of the intended meaning.
Study Variables
As this was a qualitative study, predefined quantitative variables were not measured. Instead, the study explored multiple domains related to the experiences of ASHAs in implementing community-based NCD prevention programmes. These domains included participants' understanding of their roles and responsibilities in NCD prevention, experiences with population-based screening and health promotion activities, community acceptance and participation, barriers and facilitators influencing programme implementation, adequacy of training and supportive supervision, availability of logistics and resources, experiences with digital reporting systems, motivation and job satisfaction, and recommendations for strengthening community-based NCD prevention services.
Data Analysis
Data were analysed using reflexive thematic analysis following the six-phase framework proposed by Braun and Clarke. Initially, all transcripts were read repeatedly to achieve familiarity with the data and to gain an overall understanding of participants' experiences. Meaningful units of text relevant to the study objectives were subsequently identified and assigned initial codes. Similar codes were then grouped into categories, from which broader themes and subthemes were developed through an iterative analytical process. The coding process was performed independently by two investigators to enhance analytical rigor. Differences in coding and interpretation were discussed until consensus was reached. Throughout the analysis, constant comparison of codes and themes was undertaken to ensure consistency and credibility of the findings. Representative verbatim quotations were selected to illustrate each identified theme while maintaining participant anonymity. Data analysis was performed using NVivo software. The trustworthiness of the study was ensured by adhering to the criteria proposed by Lincoln and Guba. Credibility was enhanced through prolonged engagement with the data, member checking, and investigator triangulation. Dependability was maintained through systematic documentation of methodological decisions and maintenance of an audit trail. Confirmability was strengthened by maintaining reflexive field notes throughout the research process, whereas transferability was facilitated by providing a detailed description of the study setting, participant characteristics, and research context. The study findings were reported in accordance with the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines.
Ethical Considerations
Ethical approval for the study was obtained from the Institutional Ethics Committee of [BLDE (DU)/IEC/1155/2024-25]. Written informed consent was obtained from all participants prior to enrolment after explaining the purpose of the study, interview procedures, voluntary nature of participation, and their right to withdraw from the study at any stage without any consequences. Participants were assured that their responses would be kept confidential and used exclusively for research purposes. To ensure anonymity, each participant was assigned a unique identification code, and all personal identifiers were removed during transcription. Audio recordings, transcripts, consent forms, and field notes were securely stored in password-protected electronic files and locked cabinets accessible only to the research team. The findings were presented in aggregate form, and anonymized quotations were used solely to support the interpretation of the themes. The study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki (2013) and the Indian Council of Medical Research (ICMR) National Ethical Guidelines for Biomedical and Health Research Involving Human Participants (2023) [13,14].
RESULTS
A total of 20 Accredited Social Health Activists (ASHAs) participated in the study. Data saturation was achieved after the 18th interview; however, two additional interviews were conducted to confirm that no new themes emerged, resulting in a final sample of 20 participants.
Socio-demographic characteristics of participants
The mean age of the participants was 36.8 ± 6.4 years (range: 26–48 years). The median duration of service as an ASHA was 8 years (interquartile range: 5–11 years). Most participants had completed secondary education and were actively involved in population-based NCD screening activities.
Table 1: Socio-demographic characteristics of ASHAs (N = 20)
|
Variable |
n (%) / Mean ± SD |
|
Age (years) |
36.8 ± 6.4 |
|
26–35 years |
9 (45.0) |
|
36–45 years |
8 (40.0) |
|
45 years |
3 (15.0) |
|
Education ≥ Secondary school |
17 (85.0) |
|
Median years of service (IQR) |
8 (5–11) |
Themes identified from thematic analysis
Thematic analysis yielded five major themes and twelve subthemes related to ASHAs’ experiences in implementing community-based NCD prevention and health promotion programmes.
Table 2: Major themes and subthemes
|
Major Theme |
Subthemes |
|
Understanding of NCD prevention |
Awareness of risk factors; Perceived importance of screening |
|
Expanding role of ASHAs |
Community mobilization; Follow-up and referral |
|
Barriers to implementation |
Workload; Logistic constraints; Digital reporting challenges |
|
Facilitators and motivation |
Community trust; Support from health staff; Sense of social contribution |
|
Recommendations for programme improvement |
Additional training; Better incentives; Improved supplies |
Theme 1: Understanding of NCD prevention
Most participants demonstrated a good understanding of common NCDs and their risk factors. ASHAs frequently identified high blood pressure, diabetes, unhealthy diet, tobacco use, and physical inactivity as major health concerns in their villages. Many participants perceived screening activities as important for early detection and prevention.
“Earlier people came to the hospital only when they became very sick. Now we try to identify blood pressure and sugar problems early.”
— Participant 07
Theme 2: Expanding role of ASHAs
Participants described that their responsibilities had expanded considerably beyond maternal and child health. They reported conducting household visits, motivating adults to attend screening camps, recording blood pressure and blood sugar measurements, and facilitating referrals to health facilities.
“Our work is no longer limited to pregnant women and children. We also have to identify people with BP, diabetes, and other diseases.”
— Participant 12
Theme 3: Barriers to implementation
All participants reported multiple challenges in implementing NCD-related activities. The most frequently mentioned barriers included increased workload, shortage of equipment and supplies, difficulties in using digital applications, and irregular incentives.
Table 3: Frequently reported barriers (N = 20)
|
Barrier |
Participants reporting n (%) |
|
Increased workload |
18 (90.0) |
|
Shortage of equipment/supplies |
16 (80.0) |
|
Digital reporting difficulties |
14 (70.0) |
|
Irregular incentives |
13 (65.0) |
|
Limited community participation |
11 (55.0) |
“Sometimes the machine is not available, and people get frustrated when we ask them to come again.”
— Participant 03
“There are many programmes, many registers, and now mobile reporting also takes time.”
— Participant 15
Theme 4: Facilitators and motivation
Despite challenges, participants reported several factors that helped them continue their work. Community trust, supportive supervisors, and the feeling of contributing to villagers’ health were commonly mentioned.
“People in my village know me and listen to me. That makes the work easier.”
— Participant 09
Theme 5: Recommendations for programme improvement
Participants suggested more practical training, timely incentives, regular supply of screening equipment, simplified digital reporting systems, and increased community awareness activities to strengthen NCD prevention programmes.
“If we receive regular training and proper support, we can do much better work for NCD prevention.”
— Participant 18
Visual representation of themes
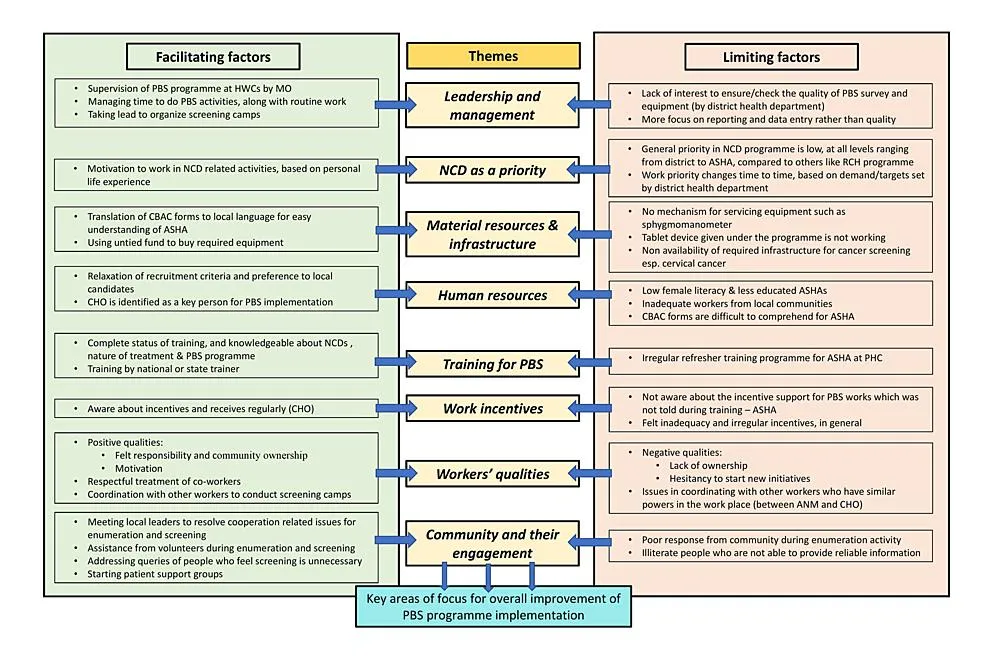
Figure 1. Conceptual framework of themes emerging from the study
DISCUSSION
The present qualitative study explored the experiences of Accredited Social Health Activists (ASHAs) in implementing community-based non-communicable disease (NCD) prevention and health promotion programmes in a rural setting. Five overarching themes emerged from the analysis: understanding of NCD prevention, expanding roles and responsibilities, barriers to programme implementation, facilitators and motivators, and recommendations for strengthening NCD services. Overall, the findings demonstrated that ASHAs possessed a satisfactory understanding of NCD prevention and recognized their pivotal role in promoting healthy lifestyles and facilitating early detection through population-based screening. However, their effectiveness was constrained by increased workload, inadequate logistics, challenges in digital reporting, and irregular incentives. Despite these barriers, community trust, supportive supervision, and intrinsic motivation enabled them to continue delivering essential preventive services.
Theme 1: Understanding of NCD Prevention
Most participants demonstrated adequate awareness of common NCDs and their behavioural risk factors, including unhealthy diet, tobacco use, physical inactivity, obesity, hypertension, and diabetes. Participants also recognized the importance of early detection and community-based screening in reducing disease complications. These findings reflect the increasing emphasis placed on NCD prevention under India's National Programme for Prevention and Control of Non-Communicable Diseases (NP-NCD), where ASHAs serve as frontline health educators and facilitators of preventive care. The findings are consistent with a recent qualitative study conducted across three Indian states, which reported that ASHAs possessed reasonable knowledge regarding cancer prevention and screening but expressed the need for periodic refresher training to improve confidence in counselling community members [15]. Similar observations have been reported from rural Karnataka, where ASHAs acknowledged their growing responsibility in identifying chronic diseases and educating communities regarding preventive health behaviours [16]. A systematic review further concluded that community health workers contribute significantly to improving awareness and promoting healthy behaviours for NCD prevention, particularly when supported by structured training and supervision [17].
Theme 2: Expanding Roles and Responsibilities
Participants consistently described a substantial expansion in their responsibilities beyond traditional maternal and child health services. They reported active involvement in household visits, population-based screening, risk assessment, health education, referral of high-risk individuals, treatment follow-up, and lifestyle counselling. These findings reflect the evolving role of ASHAs within comprehensive primary healthcare and the Ayushman Bharat initiative. Previous qualitative studies similarly describe ASHAs as essential intermediaries between communities and the formal healthcare system. Their close relationship with community members facilitates trust, improves health-seeking behaviour, and enhances participation in preventive programmes [16,18]. The expanding responsibilities observed in the present study are also consistent with research from urban Punjab, which highlighted that ASHAs have transitioned from disease-specific workers to multipurpose community health workers responsible for a broad spectrum of public health activities [18].
Theme 3: Barriers to Programme Implementation
One of the most prominent findings of this study was the range of operational barriers experienced by ASHAs during programme implementation. Increased workload, inadequate availability of screening equipment, digital reporting challenges, irregular incentives, and limited community participation emerged as major constraints affecting service delivery. These findings are consistent with several qualitative investigations conducted in India. A recent study reported that ASHAs frequently experience cognitive overload due to simultaneous responsibilities, fragmented documentation, and unreliable digital systems, ultimately affecting their efficiency and job satisfaction [19]. Likewise, studies exploring ASHAs' experiences in mental health interventions and urban health programmes have identified excessive workload, administrative burden, inadequate remuneration, and insufficient supportive supervision as important barriers influencing programme implementation [16,18]. Similar operational challenges have also been documented during implementation of population-based screening programmes under NP-NCD, where shortages of logistics and human resources limited programme effectiveness [20]. An important finding of the present study was participants' concern regarding digital reporting systems. Although digital applications improved documentation and monitoring, many ASHAs reported difficulties related to internet connectivity, application performance, and increased documentation time. Similar observations have recently been reported in qualitative studies examining digital health implementation among community health workers in India, suggesting that technology should complement rather than increase the workload of frontline workers [19].
Theme 4: Facilitators and Motivators
Despite the challenges encountered, participants identified several factors that facilitated effective programme implementation. Community trust, supportive relationships with Auxiliary Nurse Midwives (ANMs) and Medical Officers, opportunities for capacity building, and personal satisfaction derived from serving the community emerged as major motivators. These findings corroborate previous qualitative evidence demonstrating that supportive supervision, continuous mentoring, and recognition from both communities and healthcare providers substantially improve ASHAs' motivation and performance [16,18]. The strong rapport established between ASHAs and community members has consistently been identified as one of the greatest strengths of the Indian community health worker programme, enabling greater acceptance of preventive interventions and improved healthcare utilization [21].
Theme 5: Recommendations for Strengthening Community-Based NCD Prevention
Participants emphasized the need for regular refresher training, adequate availability of screening equipment, timely incentives, simplified reporting systems, and increased community awareness activities. These recommendations are highly relevant to strengthening implementation of NP-NCD services at the primary healthcare level. Comparable recommendations have emerged from recent qualitative studies involving ASHAs across India, where participants highlighted continuous professional development, supportive supervision, and recognition of their contributions as critical factors for improving programme performance [15,19]. Evidence from systematic reviews further indicates that structured training, supportive health systems, and adequate logistical support substantially enhance the effectiveness of community health worker-led NCD interventions [17].
Implications for Public Health Practice
The findings of the present study have important implications for strengthening community-based NCD prevention programmes in India. Given the expanding responsibilities of ASHAs under NP-NCD, investment in competency-based training, supportive supervision, digital infrastructure, and uninterrupted supply of screening equipment is essential. Simplifying digital reporting systems and ensuring timely financial incentives may improve job satisfaction and programme efficiency. Furthermore, strengthening collaboration between ASHAs, primary healthcare teams, and local community leaders may enhance community participation and improve the effectiveness of health promotion activities. These measures could contribute to improved coverage of population-based screening and facilitate progress toward national NCD control targets.
Strengths and Limitations
Qualitative study design provided an in-depth understanding of ASHAs' experiences, perceptions, and contextual challenges. The use of semi-structured interviews, purposive sampling, achievement of data saturation, and adherence to the COREQ reporting guidelines enhanced the credibility and trustworthiness of the findings. However, the study has certain limitations. It was conducted in the rural field practice area of a single medical college, which may limit the transferability of findings to other geographical settings. As the study relied on self-reported experiences, responses may have been influenced by recall and social desirability biases. Nevertheless, the rich qualitative data provide valuable insights into programme implementation that can inform future research and policy.
CONCLUSION
The present study demonstrated that ASHAs play a central role in implementing community-based NCD prevention and health promotion programmes. Although participants exhibited good awareness of NCD prevention and expressed strong commitment to community service, their performance was influenced by operational barriers including workload, logistical constraints, digital reporting challenges, and irregular incentives. Strengthening training, supportive supervision, resource availability, and health system support will be essential to optimize the contribution of ASHAs toward achieving national targets for NCD prevention and control.
DECLARATIONS
Patient consent for publication
Written informed consent was obtained from all participants prior to enrollment in the study.
Ethical approval: Taken
[BLDE (DU)/IEC/1155/2024-25] by BLDE (DU) Shri B M Patil Medical College, Hospital & Research Centre, Vijayapura, Karnataka.
Authors Contribution
All authors have contributed equally.
Financial Support and Sponsorship
No external funding was received for this study
Image permission statement
Not applicable
Conflict of Interest
There are no conflicts of interest
Declaration of Generative Ai and Ai-assisted Technologies in the writing process
The authors haven’t used any generative AI/AI assisted technologies in the writing process.
Data availability
Data that support the findings of this study would be made available upon reasonable request from the corresponding author via the email address.
REFERENCES




Subhajit Giri*, Adyasha Senapati, Shamin Eabenson, Nitish Kumar Dhal, Sobhana Subhadarsini Purohit, Exploring the Experiences of Accredited Social Health Activists (ASHAs) in Implementing Community-Based Non-Communicable Disease Prevention and Health Promotion Programmes: A Qualitative Study, Int. J. Med. Pharm. Sci., 2026, 2 (7), 488-498. https://doi.org/10.5281/zenodo.21274528
 10.5281/zenodo.21274528
10.5281/zenodo.21274528