
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Swami Vivekanand College of Pharmacy, Indore M.P
In the present research work an attempt has been made to optimize and formulate bilayer tablet of saxagliptin and repaglinide to achieve immediate release of saxagliptin and sustained release of repaglinide. Saxagliptin is DPP-4 inhibitor and belonging to BCS class 1 (high solubility, high permeability). It is rapidly absorbed after oral administration. It has long half life so an attempt was made to achieve its fast action by making immediate release tablet by using superdisintegrant sodium starch glycolate. Different concentration of sodium starch glycolate were used to optimize formula and it was concluded that the optimized formula SG7 sodium starch glycolate release drug 97.9 % within 30 minutes. Repaglinide is an oral blood glucose-lowering drug of the maglitinide class used in the management of type 2 diabetes mellitus. It is absorbed by oral route and has short half life, so an attempt has been done to make sustained release tablet of repaglinide And it was concluded that the optimized formula RG4 (75 mg) drug (98.6 %) in 12 hrs.
Diabetes Mellitus
Diabetes mellitus is a chronic metabolic disorder, resulting from insulin deficiency, characterized by abnormal increase in the blood sugar level, altered metabolism of carbohydrates, protein and lipids, and an increased risk of vascular complications. [1,2] Uncontrolled hepatic glucose output and reduced uptake of glucose by skeletal muscle with reduced glycogen synthesis leads to hyperglycemia. [3] As per World Health Organization, Diabetes mellitus is a chronic metabolic disorder characterized by common symptoms chronic hyperglycemia with disturbance of carbohydrate, fat and protein metabolism.It is a metabolic disorder characterized by hyperglycaemia, glycosuria, hyperlipidaemia, negative nitrogen balance and sometimes ketonaemia [4,5,6] There are numerous pathogenic processes involved in the development of diabetes. This involves autoimmune destruction of the β-cells of the pancreas which causes insulin deficiency and irregularities that result in resistance to insulin action. Deficiency of insulin on target tissues causes abnormalities in carbohydrate, fat, and protein metabolism. It may be due to inadequate insulin secretion and/or diminished tissue responses to insulin. [1, 2]
1.1 Pathophysiology of Diabetes Mellitus
The pathophysiology of diabetes depends on knowledge of the basics of carbohydrate metabolism and insulin action. Carbohydrates from the food are broken down into glucose molecules in the gut and this glucose is absorbed into the bloodstream, increasing the blood glucose levels which results in the secretion of insulin from the pancreatic beta cells. Insulin binding to specific cellular receptors facilitates entry of glucose into the cell. The cell uses glucose for energy production. The increased insulin secretion from the pancreas and the subsequent cellular utilization of glucose results in decrease of blood glucose levels. Less glucose levels in turn results in reduce insulin secretion. If insulin production and secretion are altered by diseases, blood glucose dynamics will also change. The decrease in insulin production may inhibit glucose entry into the cells resulting in hyperglycemia. Inadequate utilization of pancreatic insulin by the cells also leads to abnormal increase in the blood sugar level. When there is an elevation in the insulin secretion, blood glucose level becomes low (hypoglycemia) as large amounts of glucose enters the cells and little remains in the bloodstream. [5]
MATERIAL AND METHOD:
Table No 1: List of material used
|
S. No. |
Material Used |
Manufacturer name |
|
1. |
Saxagliptin |
Century pharmaceuticals Ltd Vadodara, Gujarat |
|
2. |
Repaglinide |
Torrent Pharma Gujarat |
|
3. |
Sodium Starch glycolate |
Lobachem Pvt. Ltd. |
|
4. |
Microcrystalline Cellulose |
Lobachem Pvt. Ltd |
|
5. |
Magnesium Stearate |
Lobachem Pvt. Ltd |
|
6. |
Talk |
Lobachem Pvt. Ltd |
|
7. |
Povidone k30 |
Lobachem Pvt. Ltd |
|
8. |
Mg stearate |
Lobachem Pvt. Ltd |
|
9. |
Sodium Stearyl fumarate |
Lobachem Pvt. Ltd |
|
10. |
Silica Gel G |
Lobachem Pvt. Ltd |
|
11. |
Methanol |
Lobachem Pvt. Ltd |
|
12. |
Ammonia |
Lobachem Pvt. Ltd |
|
13. |
Potassium chloride |
Lobachem Pvt. Ltd |
|
14. |
Hydrochloric acid |
Lobachem Pvt. Ltd |
|
15. |
Glacial acetic acid |
Lobachem Pvt. Ltd |
|
16. |
Potassium Dihydrogen Phosphate |
Merck |
Tablet No..2: List of Instrument used
|
S. No. |
Instrument used |
Make and Model |
|
1. |
UV/ visible spectrophotometer |
Schimadzu 1800 |
|
2. |
Bulk density apparatus |
Esico International 951 |
|
3. |
Magnetic stirrer |
Remi 1 MLH |
|
4. |
Humidity chamber |
Lab tech MTL-09 |
|
5. |
Dissolution apparatus |
Electro lab Pvt. Ltd. |
|
6. |
Hardness tester |
Monsanto Labs Pvt. Ltd. |
|
7. |
Vernier caliper |
P.K. Scientific |
|
8. |
Friability apparatus |
Scientech Pvt. Ltd. |
|
9. |
Disintegration apparatus |
Scientech Pvt. Ltd. |
|
10 |
Hot air Oven |
Jindal, S.M. scientific instrument Pvt. Ltd. |
|
11. |
Tablet compression machine |
Aid mach Pvt. Ltd. |
|
12. |
Weight balance |
Shimadzu ELB 800 |
|
13. |
Sonicator |
Lifecare Pvt. Ltd. |
|
14. |
pH-Meter |
Syntronics MK VI |
Preformulation study:
Drug chacterization:
Determination of λmax Saxagliptin
Preparation of calibration curve: 0.2, 0.4, 0.6, 0.8, 1,1.2, 1.4, 1.6, 1.8, 2.0 ml was pipetted out from standard stock solution (2) and diluted to 10ml with distilled water to give the final concentration of 2, 4, 6, 8, 10, 12, 14, 16, 18, 20μg/ml respectively. Absorbance at λmax against distilled water as a blank was taken and the calibration curve was plotted.
Repaglinide
Preparation of standard stock solution of repaglinide: Repaglinide (100mg) was accurately weighed and transferred into a 100ml volumetric flask. And make up the volume up to 100 ml with methanol to obtain a standard stock solution of drug concentration of 1000μg/ml.
Determination of λmax of repaglinide: From the above standard stock solution of repaglinide 250μg/ml was prepared by pipetting 2.5 ml of stock solution to a 10ml volumetric flask and making it up to 10 ml with distilled water to obtain 250μg/ml. 250μg/ml solution of repaglinide was taken and it was scanned in the range of 200-400 nm by UV spectrophotometer against distilled water as blank.
Preparation of calibration curve
Preparation of calibration curve of repaglinide in methanol
Standard stock solution (1): Repaglinide (100 mg) was accurately weighed and transferred into a 100 ml volumetric flask and the volume was made up to 100ml using methanol to obtain a standard stock solution of drug concentration of (1000μg/ml).
Standard stock solution (2): From the above standard stock solution of repaglinide100μg/ml was prepared by pipetting 1 ml of stock solution to a 10ml volumetric flask and making it up to 10 ml with distilled water.
Preparation of calibration curve: 0.25, 0.5, 0.75, 1, 1.25, 1.5, 1.75, 2, 2.25, 2.5 ml was pipetted out from standard stock solution (2) and diluted to 10 ml distilled water to give the final concentration of 2.5, 5, 7.5, 10, 12.5, 15, 17.2, 20, 22.5, 25μg/ml respectively. Absorbance at λmax against distilled water as a blank was taken and the calibration curve was plotted.
Preparation of calibration curve in 0.1 N HCl Solution
Standard stock solution (1): Repaglinide (100 mg) was accurately weighed and transferred into a 100 ml volumetric flask and dissolved and the volume was making up to 100ml using 0.1N HCl solution to obtain a standard stock of drug concentration of 1000μg/ml.
Standard stock solution (2): From the above standard stock solution of repaglinide 100μg/ml was prepared by pipetting 1 ml of stock solution to a 10ml volumetric flask and making it up to 10ml with 0.1 HCl solution.
Preparation of calibration curve: 0.2, 0,4, 0.6, 0.8, 1, 1.2, 1.4, 1.8, 2.0ml was pipette out from standard stock solution and diluted to 10 ml with 0.1N HCl solution to given the final concentration of 2, 4, 6, 8, 1, 12, 14, 16, 18, 20μg/ml respectively. The absorbance at λmax against 0.1 N HCl Solution as a blank was taken and the calibration curve was plotted.
Preparation of calibration curve of saxagliptin in buffer
Preparation of pH 1.2 hydrochloric acid: Placed 50.0 ml of the 0.2 M potassium chloride in a 200ml volumetric flask, added 85.0 ml of 0.2 M hydrochloric acid and then added water to make up the volume.
Standard stock solution (1): Saxagliptin (100mg) was accurately weighed and transferred into a 100ml volumetric flask, and dissolved and the volume was made up to 100ml using pH 1.2 hydrochloride acid to obtain a standard stock solution of drug concentration of 1000μg/ml.
Standard stock solution (2): From the above standard stock solution of saxagliptin 100μg/ml was prepared by pipetting 1 ml of stock solution to a 10ml volumetric flask and making it up to 10ml pH 1.2 hydrochloric acid.
Preparation of calibration curve: 0.2, 0.4, 0.6, 0.8, 1, 1.2, 1.4, 1.6, 1.8, 2.0ml was pipetted out and diluted to 10 ml with pH 1.2 hydrochloric acid to give the final concentration of 2, 4, 6, 8, 10,12, 14, 16, 18, 20μg/ml respectively. then absorbance at λmax against pH 1.2 hydrochloride acid as a blank was taken and the calibration curve was plotted.
Preparation of pH 6.8 phosphate buffer: Taken50 ml of 0.2 M potassium dihydrogen phosphate in a 200 ml volumetric flask. then add 22.4 ml of 0.2 M sodium hydroxide and then add water to make up the volume.
Standard stock solution (1): Saxagliptin (100 mg) was accurately weighed and transferred into a 100ml volumetric flask and dissolved and the volume was made up to 100 ml using PH 6.8 phosphate buffer to obtain a standard stock solution of drug concentration of (1000μg/ml).
Standard stock solution (2): From the above standard stock solution of saxagliptin 100μg/ml was prepared by 1 ml of stock solution to a 10ml volumetric flask and volume was made up to 10 ml pH 6.8 phosphate buffer.
Preparation of calibration curve: 0.5, 1, 1.5, 2, 2.5, 3, 3.5, 4, 4.5, 5ml was pipetted out from standard stock solution and diluted to 10ml 6.8 phosphate buffer to give the final concentration of 5, 10, 15, 20, 25, 30, 40, 40, 45,50μg/ml. and the absorbance at λmax against pH 6.8 phosphate buffer as a blank was taken and the calibration curve was plotted.
Preparation of calibration curve of repaglinide:
Preparation of calibration curve of repaglinide in methanol
Accurately weighed 100mg of repaglinide and dissolved in 100ml of methanol to make the concentration 1000μg/ml. From the above solution 0.5, 1, 1.5, 2, 2.5, 3, 3.5, 4, 4.5, 5ml was pipetted out and diluted to 10ml with methanol to give the final concentration of 50, 100, 150, 300, 350, 400, 500μg/ml respectively. And the absorbance at λmax against methanol as a blank was taken and the calibration curve was plotted.
Preparation of calibration curve of repaglinide in 0.1N HCl solution:
Accurately weighed 100mg of repaglinide and dissolved in 100ml of water to make the concentration 1000μg/ml. From the above solution 0.5, 1, 1.5, 2, 2.5, 3, 3.5, 4, 4.5, 5ml was pipetted out and diluted to 10ml with 0.1N HCl solutions to give the final concentration of 50, 100, 150, 200, 350, 400, 450, 500μg/ml respectively. Then take the absorbance at λmax against 0.1N HCl solution as a blank and the calibration curve was plotted.
Preparation of calibration curve of repaglinide in buffer:
Preparation of pH 6.8 phosphate: Placed 50.0 ml of 0.2 M potassium dihydrogen phosphate in a 200 ml volumetric flask. Added 22.4ml of 0.2 M sodium hydroxide and then added water to make up the volume.
Preparation of pH 1.2 hydrochloric acid: Placed 50.0 ml of the 0.2 M potassium chloride in a 200 ml of volumetric flask, added 85.0 ml of 0.2 M hydrochloric acid and then added water to make up the volume.
Preparation of calibration curve: Accurately weighed 100 mg of repaglinide and dissolved in 100ml of pH 6.8 phosphate buffer and pH 1.2 hydrochloric acid to make the concentration 1000μg/ml. From the above solution 0.5, 1, 1.5, 2, 2.5, 3, 3.5, 4, 4.5, 5ml was pipetted out and diluted to 10 ml with pH 6.8 phosphate buffer and pH 1.2 hydrochloric acid respectively to give the final concentration of 50,100,150, 200, 250, 300, 350, 400, 450, 500μg/ml respectively. And the absorbance at λmax against pH 6.8 phosphate buffer and pH 1.2 hydrochloric acid buffer respectively as a blank taken and the calibration curve was plotted.
Determination of the solubility
Determination of the solubility of saxagliptin and repaglinide:
Saturation shake flask method: Solubility of the samples at different pH and 0.1 N HCl solution, water was determined by the saturation shake-flask method. The sample was added to the 0.1 N HCl solution and buffer (pH 1.2 hydrochloric acid buffer and pH 6.8 phosphate buffer) and water until a heterogeneous system was obtained at 25°c temperature. The solution containing solid excess of the sample was stirred for a period of 6 hours (saturation time) at controlled temperature allowing it to achieve thermodynamic equilibrium. After further 18 hours of sedimentation, the concentration of the saturated solution was measured by UV spectroscopy.
Drug excipients interaction study
Drug excipient interaction study of saxagliptin and repaglinide: The physical mixture of drug were prepared in1:1 ratio and then passed through sieve #30. Sample of drug saxagliptin and excipient were placed in vial, closed and labeled. Then the vials were stored under conditions at 50% temp and at 75% RH in humidity chamber. Physical and chemical observations of all the mixture were done an 0th day, 15th day by TLC.
Thin layer chromatography:
Preparation of the thin layer plate: The initial slurry was prepared by vigorously shaking 30 gm of the adsorbent silica gel G with 60 ml of distilled water. Glass plate (73×24 mm) was coated with layer of silica gel G. After the silica plate had dried at room temperature, they were placed in an oven for 1 hour at 110°C for activation.
Preparation and application of sample: absorbent silica gel G was used as stationary phase. A sufficient amount of each compound was dissolved in methanol to give a concentration of 5μg/ml. A glass capillary was used to spot the sample. The diameter of each spot was limited to 0.3 cm.
Preparation of solvent system: The organic solvent methanol: ammonia: glacial acetic acid (9.4:0.4:0.2 v/v/v) was used as mobile phase. Small glass tanks 100 ml was used for developing chamber. And the solvent system was poured in to developing chamber. Glass tanks were lined with filter paper for pre saturation with solvent vapor for 15-30 minutes.
Detection of spot by chemical method: The TLC plate exposed to the vapors of the detection reagent (iodine). Iodine vapors usually stain organic compounds, making spots yellow and leaving the background white.
Calculation of Rf value: Rf value calculated by following formula: Retention factor: distance travel by solute / distance travel by solvent.
Selection of excipient:
Selection of excipient for saxagliptin immediate release layer:
Table No.3 List of excipients for immediate release layer
|
S.NO. |
Name of Excipient |
Use |
|
1. |
Sodium starch glycolate |
Super disintegrating agent |
|
2. |
Microcrystalline cellulose |
Disintegrant agent |
|
3. |
Magnesium stearate |
Lubricant |
|
4. |
Talc |
Glident |
Selection of excipient for repaglinide sustained release layer:
Table no..4 List of excipients for sustained release layer
|
S.NO. |
Name of excipient |
Use |
|
1. |
HPMC K 100 |
Polymer |
|
2. |
Eudragit |
Release retardant |
|
3. |
Magnesium stearate |
Lubricant |
|
4. |
Talc |
Glidant |
Formulation and optimization of saxagliptin and repaglinide layer:
Experimental design for optimization: A two factor, three – level factorial design (32) was employed for the formulation optimization of sustained release layer of repaglinide and immediate release of saxagliptin and Microcrystalline cellulose were selected as independent variables (factor) varied at three different level: Low(-1), medium (0), and high (+1) levels and the drug release used as dependent variables (response) for repaglinide and sodium starch glycolate, and microcrystalline cellulose were selected as independent variables (factor) varied at three different level: low (-1), medium (0), and high (+1) levels. And the drug release used as dependent variables medium (0) and high (+1) level. Experimental trials were carried out at all nine possible combinations. The factors and their limit were selected based on preliminary study. The formulation composition of the factorial batches (RG1 to RG9 & SG1 to SG9) is shown in table Repaglinide sustained release layer
Table No. .5: formulation and optimization of sustained release layer of repaglinide
|
S. No. |
Name |
RG 1 |
RG 2 |
RG 3 |
RG 4 |
RG 5 |
RG 6 |
RG 7 |
RG 8 |
RG 9 |
|
1 |
Repaglinide |
500 mg |
500 Mg |
500 mg |
500 Mg |
500 mg |
500 mg |
500 Mg |
500 Mg |
500 Mg |
|
2 |
HPMC K 100 |
75 mg |
75 Mg |
75 mg |
50 Mg |
50 mg |
50 mg |
100 Mg |
100 Mg |
100 Mg |
|
3 |
Eudragit |
75 mg |
25 Mg |
50 mg |
25 Mg |
75 mg |
50 mg |
50 Mg |
75 Mg |
25 Mg |
|
4 |
Magnesium Stearate |
5 Mg |
5 mg |
5 mg |
5 Mg |
5 mg |
5 mg |
5 Mg |
5 Mg |
5 Mg |
|
5 |
Talc |
5 mg |
5 mg |
5 mg |
5 Mg |
5 mg |
5 mg |
5 Mg |
5 Mg |
5 Mg |
Saxagliptin immediate release layer:
Table No.6: Formulation and optimization of immediate release layer of saxagliptin
|
S. No. |
Name |
SG 1 |
SG 2 |
SG 3 |
SG 4 |
SG 5 |
SG 6 |
SG 7 |
SG 8 |
SG 9 |
|
1 |
Saxagliptin |
50 mg |
50 mg |
50 mg |
50 mg |
50 mg |
50 mg |
50 Mg |
50 Mg |
50 Mg |
|
2 |
Sodium starch glycolate |
20 mg |
20 mg |
20 mg |
10 mg |
10 mg |
10 mg |
30 Mg |
30 Mg |
30 Mg |
|
3 |
Microcrystalline Cellulose |
45 Mg |
15 mg |
30 mg |
15 mg |
45 mg |
30 mg |
30 Mg |
45 Mg |
15 Msg |
|
4 |
Magnesium Stearate |
2.5 mg |
2.5 mg |
2.5 mg |
2.5 mg |
2.5 mg |
2.5 mg |
2.5 Mg |
2.5 Mg |
2.5 Mg |
|
5 |
Talk |
2.5 mg |
2.5 mg |
2.5 mg |
2.5 mg |
2.5 mg |
2.5 mg |
2.5 Mg |
2.5 Mg |
2.5 Mg |
Preparation of immediate release layer of saxagliptin:
Immediate release layer of saxagliptin was prepared by direct compression method:
Shifting: Saxagliptin and other excipient (SSG, MCC) accurately weight and were shifted through sieve no #40.
Mixing: The shifting powder were thoroughly mixed for 5 minutes and again passed through sieve no #40 for maintaining uniformity of particle size.
Lubrication: Above mixture was lubricated for 2 minutes with magnesium stearate which was already passed through sieve no #60.
Evaluation of saxagliptin and repaglinide blend: Pre-compression parameter:
Bulk density = Weight of powder in gm/ Volume packed in ml
Tapped density: Tapped density was determined by bulk density apparatus. cylinder was tapped 100 times on a plane hard surface which contained loosely packed powder and volume occupied in ml was noted.
Tapped density = Weight of powder in gm/ Tapped volume in ml
Hausner’s ratio: It is the number that is related to the flow ability of powder or granules. A Hausner’s ratio of <1.25 indicates a powder that is free flowing whereas > 1.25 indicates poor flow ability.
Hausner’s ratio = Tapped density / Bulk density
Carr’s compressibility index: It is an expression of the compressibility of a granule or powder. In pharmaceutics it is an indication of flow ability of powder. A Carr’s index with value more than 25 is considered to be an indication of low flow ability and less than 25 is having good flow property. Here small the value of Carr’s index better the flow properties of powder. For example 5-15 indicates excellent, 12-16 good, 18-21 fair and > 23 poor flow.
Carr’s Index (%) = [Tapped density – bulk density / tapped density] × 100
Angle of repose: A funnel was fixed and was secured with its tip at a height (h) of 2cm above graph paper which was placed on a horizontal surface. The powder was dropped and the radius (r) was measured. Value less than 30 indicates free flowing powder and more than 40 are poor flowing powders. Angle of repose can be measured by the following equation.
θ = tan-1 (h/r) or Tan θ = h / r
Post compression parameter
Formulation, evaluation and compression of optimized bilayer tablets: Bilayer tablets were prepared by taking best formulation from both the individual layer granules of repaglinide sustained release layer and blend of saxagliptin immediate release layer were prepared by wet granulation and direct compression respectively and pre-compression evaluation were performed.
Compression of bilayer tablet: Bilayer tablet were prepared as follows:
Repaglinide granules were first introduced into die cavity, a slight compression was made and then saxagliptin blend was introduced into the die cavity followed by final compression with optimum hardness to from a bilayer tablets. Compression was made by using rotary tablets compression machine with 12 mm deep concave punches plan on both side.
Post compression Evaluation of bilayer tablet
Thickness: Thickness of the tablets was calculated by the use of vernier callipers. The tablets exhibited uniform thickness among the different formulations.
Weight variation test: Randomly selected 20 tablets and weight individually and average weight was calculated. Not more than 2 of individual weight deviate from the average weight. No tablet must differ by more than relevant percentage.
% of weight variation = Individual weight – average weight / average weight × 100
Tablet No. 7: I.P. Limits for tablet weight variation test for uncoated and Film coated tablet
|
S. No. |
Average weight of tablet (mg) |
% Difference allowed |
|
1 |
80mg or less |
± 10% |
|
2 |
More than 80mg but less than 250 mg |
± 7.5% |
|
3 |
250mg or more |
± 5 % |
Friability: Friability was determined by using Roche tablet friability apparatus for tablets with an average weight of more than 0.65gm. 10 tablets were taken and weighed accurately and placed in the drum and rotated 100 times. Removed the tablets, removed dust from them and weighed them accurately, maximum loss of weight not greater than 1.0 % is acceptable for most tablets.
% Friability = weight before test – weight after test / weight after test × 100
Hardness: Hardness of the tablet was determined by using the Monsanto hardness tester. The tablet was taken and adjusted in tester. The tablets were placed in contact with lower plunger and a zero reading was taken. Then the plunger was forced against a spring by tightening the screw until the tablet fractured. Then the force applied to crush the tablets was noted from scale.
Swelling index: The swelling behavior of repaglinide tablets was determined at 37 ± 0.5°C in phosphate buffer pH 6.8, over 6 hrs. Formulations were individually kept in a Petri dish containing 50 ml of the buffer solution. At the end of the specific period the tablet was removed, blotted with a tissue paper and weighed. The extent of swelling was calculated by following formula.
Swelling index: weight after swelling-weight before swelling / weight before swelling × 100
Drug content: 10 tablets were weight and powder. Then accurately a quantity of the powder containing about 0.1 gm of sample substances was taken and shake with 70 ml water for 15 minutes, diluted to 100 ml with water and filter. Than diluted 1 ml of filtrate to 10 ml of water, and further diluted 1ml to10 ml with water. And absorbance of resulting solution was measured at λmax. And the drug content was calculated. Simultaneous equation method was used to determine drug content of bilayer tablet it is also called vierot’s method. If a sample contains two drugs (X and Y) each One absorbs at λmax differ from the other then it is possible to determine both drug by simultaneous equation method.
Drug release: drug release of bilayer tablets was estimated using USP type II dissolution apparatus (paddle) according to method describe in Indian pharmacopeia as follows
Method: 1000 ml of 0.1 M hydrochloric acid was placed in the vessel and the apparatus was assembled. The temperature at 36.5°C to 37.5°C and paddle speed 100 rpm was maintained. Than the dosage form was placed in the apparatus and sample volume was taken and replaced with same media. Then after 2 hrs drained the acid from the vessel and add 1000 ml pH 6.8 phosphate buffer that has previously been warmed to 36.5°C to 37.5°C and then operate at same operation as previous.
Stability study: stability study of tablets was determined physically by its visual appearance and chemical stability by thin layer chromatography using methanol: ammonia: chloroform as a solvent system. Bilayer tablets was placed in humidity chamber at the temperature 50°C and humidity 75% and room temperature for 2 months and TLC was carried out at different time interval and Rf value was calculated.
RESULTS AND DISCUSSION:
Preformulation
Drug characterization
Determination of wavelength using UV spectrophotometric analysis:
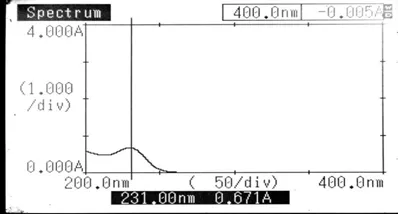
Figure No.1: lambda max of repaglinide
Preparation of calibration curve:
The calibration curve of repaglinide: The calibration curve of repaglinide in methanol pH 6.8 phosphate buffer and 0.1N hydrocloric acid was prepared and show below:
Absorbance data of repaglinide in methanol for preparation of calibration curve at 231nm.
Table No.8 Absorbance data repaglinide in methanol
|
S. No. |
Concentration (μg/ml) |
Absorbance (Mean ± standard deviation) |
|
1 |
2.5 |
0.164 ± 0.018 |
|
2 |
5 |
0.288 ±0.013 |
|
3 |
7.5 |
0.431 ±0.015 |
|
4 |
10 |
0.588 ±0.008 |
|
5 |
12.5 |
0.713 ±0.020 |
|
6 |
15 |
0.861 ±0.009 |
|
7 |
17.5 |
0.983 ±0.014 |
|
8 |
20 |
1.112 ±0.004 |
|
9 |
22.5 |
1.245 ±0.009 |
|
10 |
25 |
1.432 ±0.015 |
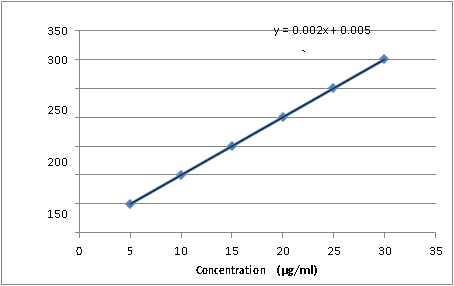
Fig.no. 2 absorbance data of repaglinide in methanol
follows Beer-Lambert’s low in the concentration Range 2.5 – 25 μg/ml.
Absorbance data of repaglinide in 0.1 N HCl Solution for preparation of calibration curve at 231 nm.
Table No 9: Absorbance data of repaglinide in 0.1 N HCl Solution.
|
S. No. |
Concentration (μg/ml) |
Absorbance (Mean ± standard deviation) |
|
1 |
50 |
0.297±0.007 |
|
2 |
100 |
0.396±0.016 |
|
3 |
150 |
0.544±0.010 |
|
4 |
200 |
0.625±0.012 |
|
5 |
250 |
0.812±0.007 |
|
6 |
300 |
0.898±0.012 |
|
7 |
350 |
1.054±0.008 |
|
8 |
400 |
1.164±0.011 |
|
9 |
450 |
` 1.325±0.009 |
|
10 |
500 |
1.465±0.002 |
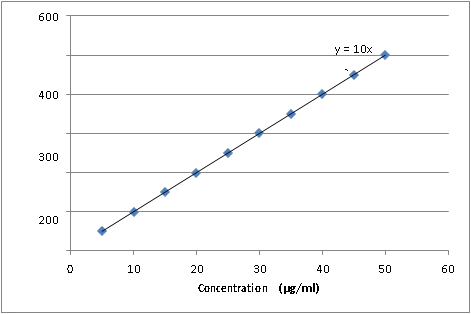
Fig.no.3 absorbance data of repaglinide in 0.1N HCL solution
Absorbance data of repaglinide in pH 1.2 hydrochloric acid for preparation of calibration curve at231 nm.
Table No 10: Absorbance data of repaglinide in pH 1.2 buffer
|
S. No. |
Concentration (μg/ml) |
Absorbance (mean ± standard deviation) |
|
1 |
5 |
0.221±0.009 |
|
2 |
10 |
0.415±0.013 |
|
3 |
15 |
0.521±0.021 |
|
4 |
20 |
0.671±0.009 |
|
5 |
25 |
0.832±0.015 |
|
6 |
30 |
0.946±0.020 |
|
7 |
35 |
1.019±0.028 |
|
8 |
40 |
1.190±0.023 |
|
9 |
45 |
1.249±0.007 |
|
10 |
50 |
1.399±0.018 |
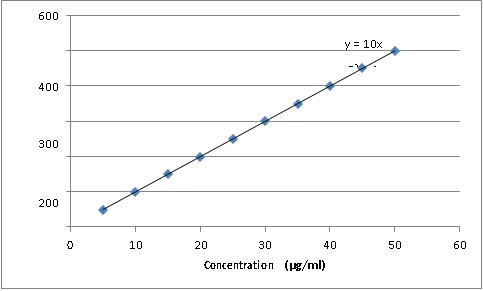
Fig.no.4 absorption data of repaglinide in 1.2 buffer
Absorbance data of repaglinide in 6.8 pH buffer for preparation of calibration curve at 231 nm
Table No. 11: Absorbance data of repaglinide in 6.8 pH buffer
|
S. No. |
Concentration (μg/ml) |
Absorbance (mean ± standard deviation) |
|
1 |
5 |
0.138±0.014 |
|
2 |
10 |
0.366±0.010 |
|
3 |
15 |
0.473±0.011 |
|
4 |
20 |
0.604±0.011 |
|
5 |
25 |
0.771±0.011 |
|
6 |
30 |
0.863±0.012 |
|
7 |
35 |
0.998±0.012 |
|
8 |
40 |
1.126±0.013 |
|
9 |
45 |
1.327±0.012 |
|
10 |
50 |
1.462±0.008 |
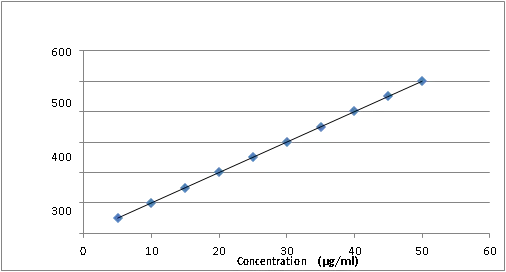
Fig.no.5 absorption data of repaglinide in 6.8 PH buffer
The calibration curve of Saxagliptin: The calibration curve of saxagliptin in distilled water, 0.1 N HCl and buffers e.g. pH 1.2 hydrochloric acid pH 6.8 phosphate was prepared and show below:
Absorbance data of saxagliptin in water for preparation of calibration curve at 208 nm:
Table No 12: Absorbance data of saxagliptin in water
|
S. No. |
Concentration (μg/ml) |
Absorbance (mean ± standard deviation) |
|
1 |
2 |
0.137 ± 0.014 |
|
2 |
4 |
0.260 ± 0.011 |
|
3 |
6 |
0.373 ± 0.015 |
|
4 |
8 |
0.537 ± 0.006 |
|
5 |
10 |
0.710 ± 0.005 |
|
6 |
12 |
0.954 ± 0.009 |
|
7 |
14 |
0.972 ± 0.021 |
|
8 |
16 |
1.169 ± 0.009 |
|
9 |
18 |
1.349 ± 0.017 |
|
10 |
20 |
1.488 ± 0.014 |
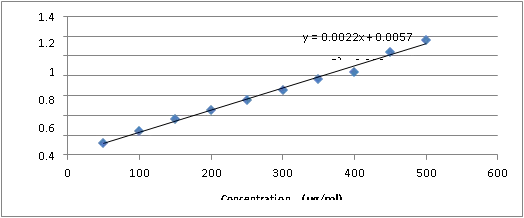
Fig.no.6 absorption data of saxagliptin in water
Absorbance data of saxagliptin in 0.1 N HCl Solution for preparation of calibration curve at 208 nm
Table No 13: Absorbance data of saxagliptin in 0.1 N HCl Solution
|
S. No. |
Concentration (μg/ml) |
Absorbance (mean ± standard deviation |
|
1 |
2 |
0.167 ± 0.004 |
|
2 |
4 |
0.234 ± 0.011 |
|
3 |
6 |
0.396 ± 0.020 |
|
4 |
8 |
0.592 ± 0.051 |
|
5 |
10 |
0.698 ± 0.016 |
|
6 |
12 |
0.869 ± 0.011 |
|
7 |
14 |
0.917 ± 0.007 |
|
8 |
16 |
1.049 ± 0.013 |
|
9 |
18 |
1.233 ± 0.007 |
|
10 |
20 |
1.350 ± 0.041 |
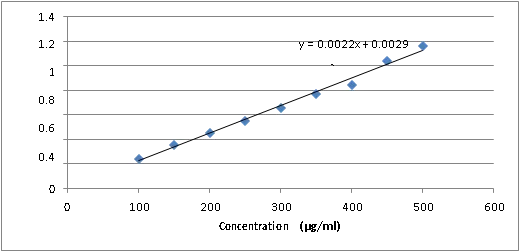
Fig.no.7Absorbance data of saxagliptin in pH 1.2 hydrochloric acid for preparation of calibration curve at 208 nm.
Table 14: Absorbance data of saxagliptin in pH 1.2 hydrochloric acid
|
S. No. |
Concentration (μg/ml) |
Absorbance (mean ± standard deviation |
|
1 |
2 |
0.157 ± 0.012 |
|
2 |
4 |
0.305 ± 0.011 |
|
3 |
6 |
0.452 ± 0.017 |
|
4 |
8 |
0.592 ± 0.010 |
|
5 |
10 |
0.754 ± 0.013 |
|
6 |
12 |
0.869 ± 0.020 |
|
7 |
14 |
0.999 ± 0.007 |
|
8 |
16 |
1.139 ± 0.011 |
|
9 |
18 |
1.243 ± 0.010 |
|
10 |
20 |
1.416 ± 0.022 |
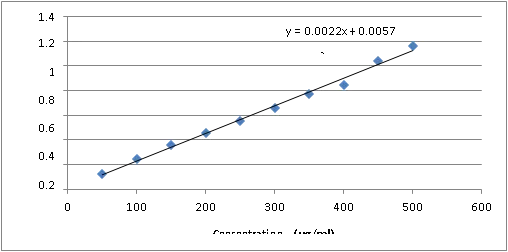
Fig.no.8 absorption of saxagliptin in PH1.2 HCL solution
Absorbance data of saxagliptin in pH 6.8 buffer for preparation of calibration curve at 208 nm.
Table No. 15: Absorbance data of saxagliptin in 6.8 pH buffer
|
S. No. |
Concentration (μg/ml) |
Absorbance (mean ± standard deviation) |
|
1 |
5 |
0.122 ± 0.011 |
|
2 |
10 |
0.243 ± 0.016 |
|
3 |
15 |
0.358 ± 0.008 |
|
4 |
20 |
0.456 ± 0.006 |
|
5 |
25 |
0.551 ± 0.018 |
|
6 |
30 |
0.660 ± 0.011 |
|
7 |
35 |
0.769 ± 0.005 |
|
8 |
40 |
0.843 ± 0.008 |
|
9 |
45 |
1.043 ± 0.015 |
|
10 |
50 |
1.165 ± 0.007 |
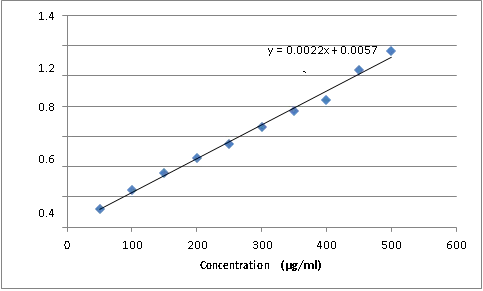
Fig. no..9 absorption of saxagliptin in PH6.8 buffer
Determination of solubility:
Solubility of drugs in various solution and buffer: The solubility of repaglinide and saxagliptin in various solution and buffer were studies and result of study shown below:
Table No. 16: solubility of drugs
|
S. No. |
Solvent |
Solubility of drug (mg/ml) (mean ± SD) |
|
|
|
|
Repaglinide |
Saxagliptin |
|
1 |
Methanol |
145.76 ± 4.06 |
174.06 ± 6.41 |
|
2 |
pH 1.2 buffer |
108.23 ± 2.39 |
144 ± 3.65 |
|
3 |
pH 6.8 buffer |
28 ± 5.87 |
3.70 ± 0.30 |
It is cleared from study that both have good solubility in different buffer and solution.
Drug excipient interaction study:
The drug was found to be compatible with various excipients which were selected for formulation of bilayer tablet the compatibility was assessed by TLC (thin layer chromatography) and the retention factor of all ratio found similar.
Table 17: List of drug excipient retention found factor
|
S. No. |
Drug Excipient Ratio (1:1) |
Initial appearance present day |
Final appearance after 15 days |
Retention factor present day |
Retention Factor After 15 days |
|
1 |
Repaglinide |
Off white Powder |
No change |
0.72 |
0.71 |
|
2 |
Repaglinide: HPMC K 100 |
White powder |
No change |
0.78 |
0.78 |
|
3 |
Repaglinide: Eudragit |
White mixture |
No change |
0.76 |
0.75 |
|
4 |
Repaglinide: Magnesium stearate |
White mixture |
No change |
0.72 |
0.70 |
|
5 |
Repaglinide: Tppalc |
White mixture |
No change |
0.76 |
0.77 |
|
6 |
Repaglinide: all excipient |
White mixture |
No change |
0.75 |
0.76 |
|
7 |
Saxagliptin |
Light yellow |
No change |
0.80 |
0.79 |
|
8 |
Saxagliptin: Sodium starch glycolate |
Light yellow |
No change |
0.88 |
0.85 |
|
9 |
Saxagliptin: MCC |
Off white |
No change |
0.82 |
0.83 |
|
10 |
Saxagliptin: Magnesium stearate |
Off white |
No change |
0.87 |
0.86 |
|
11 |
Saxagliptin: Talc |
Off white |
No change |
0.79 |
0.79 |
|
12 |
Saxagliptin: all excipient |
Off white |
No change |
0.81 |
0.83 |
Formulation and optimization
All the batch of factorial design was prepared and evaluate as shown in table:
Precompression parameter: Result of precompression parameter of repaglinide granules or saxagliptin blends:
Table No. 18: Result of precompression parameter of repaglinide granules.
|
S. NO |
Formulation |
Bulk density (gm/cm3) (mean ± SD) |
Tapped density (gm/cm3) (mean ± SD) |
Carr’s index % (mean ± SD) |
Hausner’s ratio (mean ± SD) |
Angle of Repose (°) (mean ± SD) |
|
1 |
RG1 |
0.388 ± 0.02 |
0.408 ± 0.03 |
6.7 ± 1.7 |
1.06 ± 0.02 |
17.57° ± 0.7 |
|
2 |
RG2 |
0.432 ± 0.004 |
0.502 ± 0.005 |
13.8 ±0.7 |
1.14 ± 0.01 |
15.29 °± 0.61 |
|
3 |
RG3 |
0.442 ± 0.007 |
0.513 ± 0.007 |
13.17 ± 0.94 |
1.14 ± 0.01 |
16.35 °± 0.60 |
|
4 |
RG4 |
0.537 ± 0.005 |
0.594 ± 0.001 |
9.66 ± 0.91 |
1.09 ± 0.01 |
16.10°± 0.7 |
|
5 |
RG5 |
0.498 ± 0.007 |
0.540 ± 0.008 |
7.68 ± 0.13 |
1.07 ± 0.01 |
18.68° ± 0.3 |
|
6 |
RG6 |
0.496 ± 0.005 |
0.542 ± 0.005 |
8.39 ± 0.15 |
1.08 ± 0.01 |
16.04° ± 0.9 |
|
7 |
RG7 |
0.455 ± 0.010 |
0.482 ± 0.007 |
5.49 ± 2.24 |
1.04 ± 0.02 |
16.87° ± 0.1 |
|
8 |
RG8 |
0.449 ± 0.015 |
0.535 ± 0.009 |
16.01 ± 2.29 |
1.07 ± 0.03 |
24.65° ± 0.3 |
|
9 |
RG9 |
0.393 ± 0.003 |
0.479 ± 0.001 |
17.96 ± 0.67 |
1.21 ± 0.01 |
18.7° ± 0.2 |
Table No. 19: Result of precompression parameter of saxagliptin blend
|
S. No. |
Formulation |
Bulk density (gm/cm3) (mean ± SD) |
Tapped Density (gm/cm3) (mean ± SD) |
Carr’s index % (mean ± SD) |
Hausner’s ratio (mean ± SD) |
Angle of Repose (°) (mean ± SD) |
|
1 |
SG1 |
0.352 ± 0.02 |
0.434 ± 0.030 |
18.7 ± 0.73 |
1.23 ± 0.01 |
9.5 ± 0.57 |
|
2 |
SG2 |
0.420 ± 0.005 |
0.531 ± 0.006 |
19.35 ± 0.57 |
1.25 ± 0.005 |
12.2 ± 0.85 |
|
3 |
SG3 |
0.354 ± 0.04 |
0.431 ± 0.017 |
17.62 ± 0.68 |
1.22 ± 0.011 |
9.6 ± 0.86 |
|
4 |
SG4 |
0.446 ± 0.02 |
0.605 ± 0.050 |
26.06 ± 01.6 |
1.18 ± 0.11 |
10.52 ± 0.7 |
|
5 |
SG5 |
0.391 ± 0.39 |
0.461 ± 0.054 |
14.89 ± 0.98 |
1.23 ± 0.02 |
15.02 ± 0.7 |
|
6 |
SG6 |
0.318 ± 0.009 |
0.406 ± 0.026 |
24.41 ± 0.99 |
1.18 ± 0.017 |
9.59 ± 0.4 |
|
7 |
SG7 |
0.365 ± 0.008 |
0.390 ± 0.010 |
6.44 ± 0.28 |
1.34 ± 0.005 |
13.5 ± 0.6 |
|
8 |
SG8 |
0.339 ± 0.012 |
0.357 ± 0.014 |
5.27 ± 0.21 |
1.06 ± 0.003 |
14.22 ± 0.3 |
|
9 |
SG9 |
0.567 ±0.039 |
0.645 ± 0.050 |
11.96 ± 0.79 |
1.12 ± 0.017 |
15.82 ± 0.6 |
Post compression parameter
In vitro drug release of tablets: Cumulative drug release of repaglinide sustained release tablets were as follows:
Table No. 20: Cumulative % drug release of repaglinide sustained release tablet
|
S. No |
Time (hours) |
% Cumulative drug release |
||||||||
|
RG1 (Means± SD) |
RG2 (Means± SD) |
RG3 (Means± SD) |
RG4 (Means± SD) |
RG5 (Means± SD) |
RG6 (Means± SD) |
RG7 (Means± SD) |
RG8 (Means± SD) |
RG9 Means± SD) |
||
|
1 |
1 |
6.35± 0.1 |
7.9± 0.3 |
9.4± 0.3 |
12.4± 0.2 |
6.5± 0.4 |
5.78± 0.6 |
6.34± 0.1 |
4.9± 0.3 |
3.88± 0.5 |
|
2 |
2 |
10.29± 0.4 |
7.85± 0.2 |
18.8± 0.4 |
18.9± 0.4 |
12.9± 0.3 |
12.93± 0.4 |
10.27± 0.4 |
7.26± 0.29 |
6.71± 0.25 |
|
3 |
3 |
23.14± 0.8 |
22.5± 0.8 |
25.4± 0.3 |
29.0± 0.5 |
17.6± 0.8 |
23.26± 0.6 |
24.12± 0.8 |
13.23± 0.24 |
11.4± 1.2 |
|
4 |
4 |
28.16± 0.4 |
35.3± 0.7 |
36.5± 0.3 |
38.3± 0.5 |
26± 0.6 |
28.35± 1.3 |
27.15± 0.4 |
17.67± 0.34 |
22.3± 0.6 |
|
5 |
5 |
37.26± 1.0 |
39.4± 1.8 |
43.8± 1.35 |
48± 0.2 |
32.5± 1.04 |
34.12± 1.1 |
36.62± 1.2 |
24.06± 0.9 |
31.4± 0.32 |
|
6 |
6 |
50.0± 0.28 |
49± 0.5 |
52.6± 1.0 |
54.6± 1.10 |
48.4± 1.4 |
37.38± 0.5 |
42.4± 0.23 |
38.05± 0.6 |
35.5±1. 3 |
|
7 |
8 |
90.09± 0.8 |
90.9± 0.7 |
94.5± 0.9 |
98.6± 0.6 |
88.0± 1.8 |
83.23± 0.7 |
86.09± 0.8 |
85.73± 1.8 |
84.3±0. 9 |
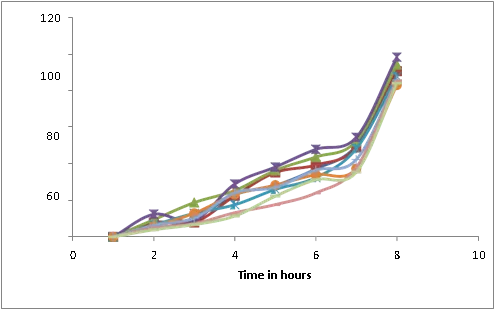
Fig. no. 10 Cumulative % drug release of repaglinide sustained release layer
From the above result of cumulative % drug release of repaglinide sustained release tablets, it was concluded, RG4 formulation shows better drug release.
Cumulative drug release of saxagliptin immediate release tablets were as follows
Table No. 21 Cumulative %drug release of saxagliptin immediate release tablet
|
S. NO. |
Time (minutes) |
%cumulative drug release |
||||||||
|
SG1 (Means± SD) |
SG2 (Means± SD) |
SG3 (Means± SD) |
SG4 (Means± SD) |
SG5 (Means± SD) |
SG6 (Means± SD) |
SG7 (Means± SD) |
SG8 (Means± SD) |
SG9 (Means± SD) |
||
|
1 |
5 |
16.8± 1.0 |
5.1± 1.0 |
16.1± 0.5 |
23.7± 1.3 |
31.8± 1.1 |
29.6± 1.3 |
44.1± 1.3 |
36.4± 1.0 |
35.5± 1.0 |
|
2 |
10 |
33.2± 1.1 |
14± 1.3 |
27.1± 1.9 |
46.2± 1.3 |
49.1± 1.0 |
53.4± 2.3 |
54.5± 1.7 |
51.5± 1.3 |
51.4± 1.3 |
|
3 |
15 |
46.1± 1.0 |
27.5± 1.4 |
44.3± 1.0 |
55.0± 2.0 |
62.1± 1.0 |
64.3± 1.4 |
61.4± 1.1 |
55.7± 1.2 |
55.7± 1.2 |
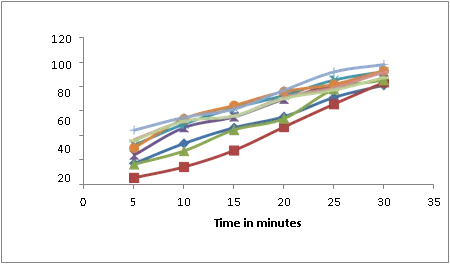
Fig. no. 11 Cumulative % drug release of Saxagliptin immediate release layer
From the above result of cumulative %drug release of saxagliptin immediate release tablets, it was concluded, SG7 formulation shows better drug release. From the study of factorial design it was found that RG4 and SG7 were best of nine formulation which were used to formulate bilayer tablet
Table No. 22: Optimized formula of individual layer of bilayer tablet
|
S. No. |
Sustained release Layer content |
Quantity |
|
1 |
Repaglinide |
500 mg |
|
2 |
HPMC K 100 |
50mg |
|
3 |
Microcrystalline Cellulose |
75 mg |
|
4 |
Magnesium stearate |
5 mg |
|
5 |
Talc |
5 mg |
|
S. No. |
Immediate release Layer content |
Quantity |
|
1 |
Saxagliptin |
50 mg |
|
2 |
Sodium starch glycolate |
45mg |
|
3 |
Microcrystalline Cellulose |
30 mg |
|
4 |
Magnesium stearate |
2.5 mg |
|
5 |
Talc |
2.5 mg |
Evaluation of bilayer tablet
Pre-compression parameter: Result of pre-compression parameters of optimized layers of bilayer tablets were as follows:
Table No. 22: precompression parameter of individual layer
|
S. No. |
Drug |
Bulk density (gm/cm3) (means ± SD) |
Tapped Density (gm/cm3) (means ± SD) |
Carr’s index % (mean ± SD) |
Hausner’s ratio (mean ± SD) |
Angle of Repose (°) (mean± SD) |
|
1 |
Repaglinide |
0.59 ± 0.02 |
0.68 ± 0.03 |
14.6 ± 0.7 |
0.8 ± 0.4 |
26 ± 0.6 |
|
2 |
Saxagliptin |
0.34 ± 0.004 |
0.42 ± 0.06 |
7.12 ± 0.5 |
1.09 ± 0.08 |
15 ± 0.7 |
Post compression parameter:
Result of optimized bilayer tablets were as follows:
Table No. 23: post compression parameter of bilayer tablet
|
S. No. |
Thickness (mean ± SD) |
Hardness (mean ± SD) |
Weight Variation(mg) (mean ± SD) |
Friability (mean ± SD) |
Drug content (mean ± SD) |
|
|
Repaglinide |
Saxagliptin |
|||||
|
1 |
5.4 ± 0.04 |
4.6 ± 0.15 |
752 ± 6.45 |
0.48 ± 0.22 |
96.32 ± 0.53 |
98.85 ± 0.5 |
Swelling index of bilayer tablet
Table No. 24: Swelling index of bilayer tablet
|
Time (hour) |
Swelling index % (mean ± SD) |
|
1 |
35.78 ± 0.6 |
|
2 |
49.85 ± 0.5 |
|
3 |
57.7 ± 0.2 |
|
4 |
65.44 ± 0.3 |
|
5 |
71.02 ± 0.5 |
|
6 |
82.78 ± 0.2 |
Swelling behavior of bilayer tablet shown in table no. 7.19 and it was observed that bilayer tablet was swelled 82.7 % within 6 hours.
In vitro drug release of bilayer tablet:
Table No.25: % cumulative drug release of bilayer tablet
|
S. No. |
Time |
% cumulative drug release of bilayer table (mean ± SD) |
|
|
Saxagliptin |
Repaglinide |
||
|
1 |
5 min |
46.3 ± 0.76 |
|
|
2 |
10 min |
58.2 ± 0.05 |
|
|
3 |
15 min |
62.4 ± 0.26 |
|
|
4 |
20 min |
84.6 ± 0.54 |
|
|
5 |
25 min |
94.2 ± 0.68 |
|
|
6 |
30 min |
96. 8 ± 0.34 |
|
|
7 |
1 hr |
|
8.4 ± 0.67 |
|
8 |
2 hr |
|
16 ± 0.68 |
|
9 |
3 hr |
|
29.2 ± 0.45 |
|
10 |
4 hr |
|
38.5 ± 0.52 |
|
11 |
5 hr |
|
49.9 ± 0.78 |
|
12 |
6 hr |
|
52 ± 0.44 |
|
13 |
8hr |
|
96.58 ± 0.27 |
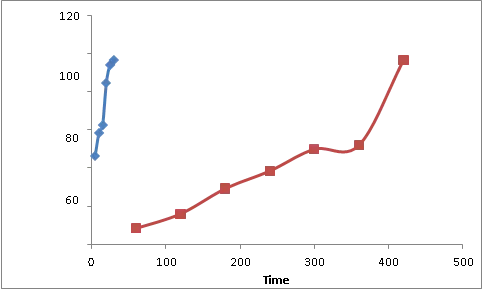
Fig no. 12: Cumulative % drug release of bilayer tablel
Drug release was determined according to procedure of Indian pharmacopoeia and results shown in table no. 7.20 and it was observed that immediate release layer of bilayer tablet release its 96.8% drug release in 30 minutes and after that sustained release layer of bilayer tablet started to release its drug and 97.96% of drug was released up to 12 hours.
Stability study of bilayer tablet: stability study for two month was performed at room temperature and temp.50°C% and humidity 75% of bilayer tablet. It was observed that there was no change in physical appearance and chemical changes were confirmed by TLC which was found similar at different time interval and at different storage conditions. From the result it was concluded that the formulation is stable at different storage condition.
Table No. 26: stability study of bilayer tablet
|
S. NO. |
Time |
Storage condition |
Physical appearance |
Rf value |
||
|
Temp |
humidity |
Repaglinide |
Saxagliptin |
|||
|
1 |
Initial |
Room temperature |
Pinkish white |
0.66 |
0.84 |
|
|
2 |
1 month |
Room temperature |
No change |
0.67 |
0.84 |
|
|
3 |
50% |
75% |
No change |
0.66 |
0.83 |
|
|
4 |
2 month |
Room temperature |
No. change |
0.64 |
0.83 |
|
|
5 |
50% |
75% |
No change |
0.67 |
0.82 |
|
SUMMARY AND CONCLUSION
In the present research work an attempt has been made to optimize and formulate bilayer tablet of saxagliptin and repaglinide to achieve immediate release of saxagliptin and sustained release of repaglinide. Saxagliptin is DPP-4 inhibitor and belonging to BCS class 1 (high solubility, high permeability). It is rapidly absorbed after oral administration. It has long half life so an attempt was made to achieve its fast action by making immediate release tablet by using superdisintegrant sodium starch glycolate. Different concentration of sodium starch glycolate were used to optimize formula and it was concluded that the optimized formula SG7 sodium starch glycolate release drug 97.9 % within 30 minutes. Repaglinide is an oral blood glucose-lowering drug of the maglitinide class used in the management of type 2 diabetes mellitus. It is absorbed by oral route and has short half life, so an attempt has been done to make sustained release tablet of repaglinide And it was concluded that the optimized formula RG4 (75 mg) drug (98.6 %) in 12 hrs. So by taking both optimized formulation in fixed dose combination in different layer a bilayer tablet was prepared with 50 mg saxagliptin and 500 mg of repaglinide which give following benefits.
Bilayer tablet has been made and evaluated. For various precompression and post compression parameter. Precompression parameter shows that the granules and blends of repaglinide and saxagliptin have good Carr’s index and hausner’s ratio indicate that both granules and blends were free flowing. The angle of repose shows that granules and blends have excellent flow and post compression parameter show that bilayer tablet have thickness hardness and weight and friability within the I. P. limit and bilayer tablet have swelling index 82% in 6 hrs and have drug release first layer of saxagliptin release 98.6 % in 30 minutes and second layer repaglinide release 95.5 % in 12 hrs.
REFERENCES

Abhishek Kumar*, Rajat Pawar, Sunita Patidar, Apurva Pagare, Dishant Gupta, Formulation and Development of Bilayer Tablet of Saxagliptin and Repaglinide, Int. J. Med. Pharm. Sci., 2026, 2 (7), 617-639. https://doi.org/10.5281/zenodo.21350201
 10.5281/zenodo.21350201
10.5281/zenodo.21350201