
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1M. Pharm 2nd yr., Department of Pharmaceutics, Dr. Vedprakash Patil Pharmacy College, Chh. Sambhajinagar, Maharashtra, India
2Assistant Professor, Department of Quality Assurance, Dr. Vedprakash Patil Pharmacy College, Chh. Sambhajinagar, Maharashtra, India
The present work aimed to formulate and evaluate colon-targeted Ozanimod tablets intended to provide localized drug release for inflammatory bowel disease. Ozanimod, a sphingosine-1-phosphate receptor modulator, may benefit from site-specific delivery because ulcerative colitis and many colonic inflammatory lesions are localized within the large intestine, whereas conventional systemic exposure can contribute to dose related adverse effects. Tablets were prepared by the wet granulation technique using Eudragit S100, Eudragit L100 and ethyl cellulose as release-modifying polymers, with microcrystalline cellulose as diluent, PVP K30 as binder, talc as glidant and magnesium stearate as lubricant. A three-level factorial design was applied to assess the influence of polymer concentration on lag time and cumulative drug release at 12 h. Preformulation studies confirmed acceptable organoleptic properties, melting point range of 132-135 °C and a UV analytical wavelength of 270 nm. FTIR spectra retained characteristic Ozanimod peaks and DSC thermograms showed no major disappearance of the drug melting transition, suggesting compatibility with selected excipients. All powder blends exhibited satisfactory flow and compressibility. Post-compression tests showed acceptable weight variation, thickness, hardness, friability and drug content. Among nine formulations, F7 containing 60 mg Eudragit S100, 20 mg Eudragit L100 and 10 mg ethyl cellulose showed the best performance with lag time of 3.2 h, drug content of 99.6% and 94% cumulative release at 12 h. Stability testing for three months showed only minor changes in tablet properties and dissolution behavior. The optimized formulation therefore demonstrated suitable delayed-release and colon-targeting potential for further in vivo evaluation.
Inflammatory bowel disease (IBD) is a chronic relapsing inflammatory disorder of the gastrointestinal tract that mainly includes ulcerative colitis and Crohn’s disease. Both conditions are associated with dysregulated immune responses, altered gut microbiota, impaired epithelial barrier function and repeated cycles of mucosal injury. Ulcerative colitis is particularly suitable for local therapy because inflammation is largely restricted to the colon and rectum, whereas Crohn’s disease may involve discontinuous lesions throughout the gastrointestinal tract. Recurrent symptoms such as abdominal pain, diarrhea, rectal bleeding, urgency, fatigue and weight loss substantially reduce patient quality of life and often require long-term pharmacotherapy. Conventional therapy for IBD includes aminosalicylates, corticosteroids, immunosuppressants, biologics and newer oral small molecules. Although these therapies improve clinical outcomes, systemic administration may lead to incomplete drug localization at inflamed colonic tissue and may increase the risk of systemic side effects. For drugs with immunomodulatory activity, minimizing unnecessary systemic exposure while maintaining therapeutic concentrations at the site of inflammation is a desirable formulation goal.
Colon-targeted drug delivery systems are designed to protect drug molecules during passage through the stomach and small intestine and release the active ingredient in the distal intestine or colon. Common approaches include pH-dependent polymers, time-dependent release systems, microflora-triggered systems and hybrid technologies. Eudragit S100 and Eudragit L100 are methacrylic acid copolymers that dissolve at different intestinal pH thresholds and can be used to delay release until the dosage form reaches higher-pH intestinal regions. Ethyl cellulose provides a hydrophobic diffusion-controlling barrier that further modifies release kinetics.
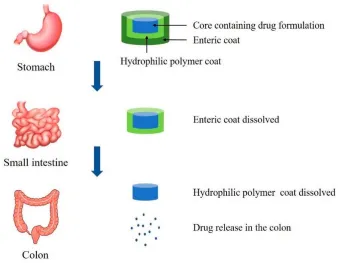
Figure 1A. Schematic representation of colon-targeted delivery showing protection in the stomach and small intestine followed by drug release in the colon.
Ozanimod is a selective sphingosine-1-phosphate receptor modulator that reduces lymphocyte migration from lymphoid tissue and thereby decreases inflammatory cell trafficking. Because the therapeutic target in ulcerative colitis is the inflamed colonic mucosa, a colon-targeted Ozanimod formulation could potentially improve local action and reduce systemic adverse effects. The present manuscript converts the thesis investigation into a research article focused on formulation design, in vitro evaluation, optimization and stability assessment of colon-targeted Ozanimod tablets.
2. MATERIALS AND METHODS
2.1 MATERIALS
Ozanimod was used as the active pharmaceutical ingredient. Eudragit S100, Eudragit L100 and ethyl cellulose were selected as pH-dependent and release-controlling polymers. Microcrystalline cellulose PH 102, PVP K30, talc and magnesium stearate were used as diluent, binder, glidant and lubricant, respectively. Methanol, ethanol, distilled water and buffer media were used for analytical and dissolution studies.
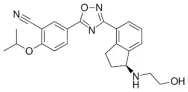
Figure 2. Chemical structure of Ozanimod used as the active pharmaceutical ingredient.
2.2 Preformulation and analytical studies
Ozanimod was evaluated for color, odor, appearance and texture. Melting point was determined using a capillary method in a digital melting point apparatus and compared with the reported value. Solubility was examined in selected aqueous and organic media after shaking for 24 h, filtration and UV-visible analysis. The UV spectrum of Ozanimod was scanned between 200 and 400 nm, and the analytical wavelength was fixed at 270 nm. Calibration standards of 2, 4, 6, 8 and 10 µg/mL were prepared, and absorbance was measured at 270 nm to construct a calibration curve.
2.3 Drug-excipient compatibility studies
Fourier-transform infrared spectroscopy was performed on pure drug and physical mixtures using the potassium bromide pellet technique over the range of 4000-400 cm⁻¹. Spectra were compared for shifting, disappearance or emergence of major functional-group peaks. Differential scanning calorimetry was performed for pure Ozanimod and drug-excipient mixtures in the range of 30-300 °C under nitrogen, using an empty aluminum pan as reference. Onset, peak, endset and enthalpy values were compared to assess thermal compatibility.
2.4 Experimental design and formulation development
A three-level factorial design was used to study the effects of Eudragit S100, Eudragit L100 and ethyl cellulose concentration on lag time and cumulative drug release at 12 h. Nine formulations were prepared by wet granulation. Ozanimod, microcrystalline cellulose and polymers were passed through sieve #60 and mixed uniformly. PVP K30 binder solution was prepared in isopropyl alcohol and added gradually to form a damp mass. The wet mass was passed through sieve #16, dried at 40 °C, passed through sieve #20 and lubricated with talc and magnesium stearate. Granules were compressed into tablets using a rotary tablet press.
Table 1. Composition of optimized colon-targeted Ozanimod tablet (F7, per tablet).
|
Ingredient |
Quantity (mg) |
Function |
|
Ozanimod |
10 |
Active pharmaceutical ingredient |
|
Eudragit S100 |
60 |
pH-dependent colon-targeting polymer |
|
Eudragit L100 |
20 |
Enteric pH-sensitive polymer |
|
Ethyl cellulose |
10 |
Hydrophobic release modifier |
|
Microcrystalline cellulose |
75 |
Diluent and compression aid |
|
PVP K30 |
5 |
Binder |
|
Talc |
2 |
Glidant/anti-adherent |
|
Magnesium stearate |
2 |
Lubricant |
2.5 Evaluation of tablets
Precompression parameters included angle of repose, bulk density, tapped density, Carr’s index and Hausner ratio. Compressed tablets were evaluated for physical appearance, weight variation, thickness, hardness, friability and drug content uniformity. Drug content was measured after powdering tablets, extracting drug in phosphate buffer pH 7.4, filtration, suitable dilution and UV-visible analysis at the predetermined wavelength.
In vitro dissolution was performed using USP Type II paddle apparatus at 37 ± 0.5 °C and 50 rpm. To simulate gastrointestinal transit, tablets were exposed to 0.1 N HCl for 2 h, phosphate buffer pH 6.8 for the next 3 h and phosphate buffer pH 7.4 until 12 h. Samples were withdrawn at predetermined intervals, filtered, diluted and analyzed spectrophotometrically. Cumulative percentage drug release was calculated and plotted against time. The optimized formulation was subjected to stability study for three months under controlled storage conditions, and changes in appearance, tablet properties, drug content, release and lag time were recorded.
3. RESULTS AND DISCUSSION
3.1 Preformulation and analytical findings
Ozanimod appeared as a white to off-white, odorless, crystalline and fine free-flowing powder. The observed melting point range was 132-135 °C, close to the reported value of 135 °C, supporting drug identity and acceptable purity. UV analysis showed maximum absorbance at 270 nm. The calibration curve was linear over the concentration range of 2-10 µg/mL, with the regression equation y = 0.0511x + 0.0344 and R² = 0.9955. This confirmed suitability of the UV method for quantitative analysis of Ozanimod during drug content and dissolution testing.
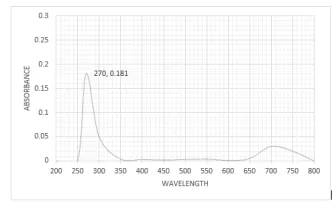
Figure 3. UV absorption spectrum of Ozanimod showing lambda max at 270 nm.
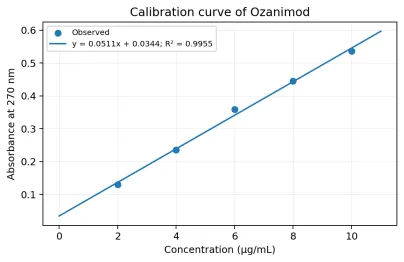
Figure 4. Calibration curve of Ozanimod at 270 nm.
3.2 Compatibility studies
The FTIR spectrum of Ozanimod showed characteristic bands corresponding to N-H stretching, aliphatic C-H stretching, nitrile C≡N stretching, aromatic C=C stretching, C-N stretching and aromatic out-of-plane C-H bending. The major peaks were retained in the drug-excipient mixture without meaningful disappearance of characteristic signals, indicating absence of major chemical interaction. DSC analysis showed a melting transition for pure Ozanimod with onset, peak and endset temperatures of 130.2, 139.6 and 149.3 °C, respectively. The physical mixture showed onset, peak and endset values of 123.2, 136.5 and 143.1 °C, respectively, with a slight decrease in enthalpy from 118 to 115 mJ. The retention of the characteristic melting behavior suggested no significant incompatibility between Ozanimod and selected excipients.
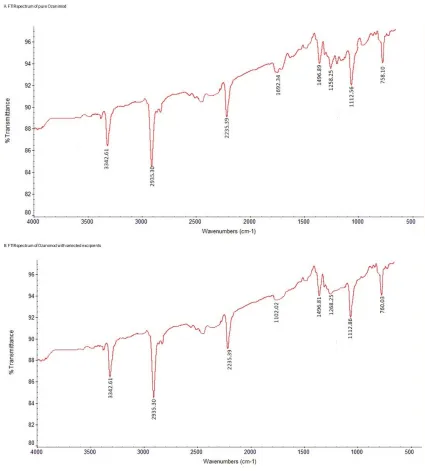
Figure 5. FTIR spectra showing retention of the major functional group peaks in the pure drug and drug excipient mixture.
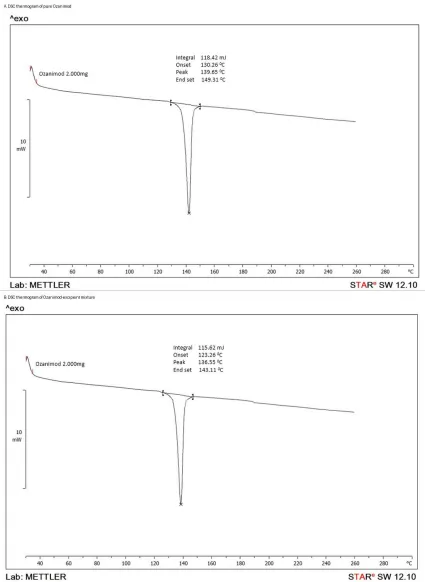
Figure 6. DSC thermograms of pure Ozanimod and the drug-excipient mixture used for compatibility interpretation.
Table 3. Selected FTIR and DSC observations used for compatibility interpretation.
|
Test |
Observation |
Interpretation |
|
FTIR |
Characteristic Ozanimod bands included 3342 cm⁻¹ (N-H), 2935 cm⁻¹ (C-H), 2231 cm⁻¹ (C≡N), 1622 cm⁻¹ (aromatic C=C), 1258 cm⁻¹ (C-N) and 758 cm⁻¹ (aromatic C-H bending). |
Retention of major peaks indicated no major chemical incompatibility. |
|
DSC |
Pure drug peak temperature was 139.6 °C; drug-excipient mixture peak temperature was 136.5 °C. |
Minor shift was attributed to dilution or physical mixing; no disappearance of drug transition was observed. |
3.3 Precompression and post-compression evaluation
All powder blends displayed satisfactory flow and compressibility. The angle of repose ranged from 27.8° to 31.2°, bulk density from 0.44 to 0.48 g/cm³, tapped density from 0.53 to 0.55 g/cm³, Carr’s index from 12.72% to 16.98% and Hausner ratio from 1.14 to 1.20. The optimized batch F7 showed the best flow characteristics with angle of repose of 27.8°, Carr’s index of 12.72% and Hausner ratio of 1.14. These properties are advantageous for uniform die filling, consistent tablet weight and reproducible drug distribution. Post-compression data indicated that all formulations were acceptable with respect to weight variation, thickness, hardness, friability and drug content. The optimized F7 formulation showed hardness of 3.3 kg/cm², friability of 0.42%, average weight of 200 mg and drug content of 99.6%. The low friability and higher hardness suggest adequate mechanical strength, while the high drug content indicates uniform distribution of Ozanimod in the tablet matrix. The complete post-compression parameter results for individual batches are presented in Table 5, showing acceptable batch-to-batch uniformity and confirming the superiority of optimized batch F7.
Table 4. Summary of tablet evaluation results.
|
Parameter |
Overall range (F1-F9) |
Optimized F7 value |
|
Bulk density (g/cm³) |
0.44-0.48 |
0.48 |
|
Tapped density (g/cm³) |
0.53-0.55 |
0.55 |
|
Angle of repose (°) |
27.8-31.2 |
27.8 |
|
Carr’s index (%) |
12.72-16.98 |
12.72 |
|
Hausner ratio |
1.14-1.20 |
1.14 |
|
Weight variation (mg) |
198-202 |
200 |
|
Thickness (mm) |
2.2-2.5 |
2.5 |
|
Hardness (kg/cm²) |
1.7-3.3 |
3.3 |
|
Friability (%) |
0.42-0.72 |
0.42 |
|
Drug content (%) |
96.5-99.6 |
99.6 |
Table 5. Post-compression parameter results of factorial batches F1-F9.
|
Batch |
Weight variation (mg) |
Thickness (mm) |
Hardness (kg/cm2) |
Friability (%) |
Drug content (%) |
|
F1 |
198 |
2.2 |
2.4 |
0.72 |
96.5 |
|
F2 |
201 |
2.3 |
2.5 |
0.70 |
97.2 |
|
F3 |
200 |
2.3 |
1.7 |
0.68 |
96.8 |
|
F4 |
202 |
2.4 |
2.9 |
0.64 |
98.1 |
|
F5 |
199 |
2.4 |
2.0 |
0.60 |
98.5 |
|
F6 |
201 |
2.5 |
2.1 |
0.58 |
99.0 |
|
F7 (Optimized) |
200 |
2.5 |
3.3 |
0.42 |
99.6 |
|
F8 |
198 |
2.4 |
2.8 |
0.55 |
98.2 |
|
F9 |
199 |
2.3 |
1.7 |
0.61 |
97.6 |
F7 was selected as the optimized formulation because it showed the highest hardness (3.3 kg/cm2), lowest friability (0.42%), ideal tablet weight (200 mg) and maximum drug content (99.6%).
Design of Experiment
The DOE contour and 3D surface plots show the combined effect of Eudragit S100 and Eudragit L100 on the lag time and drug release of Ozanimod colon-targeted tablets. The contour plot for lag time indicates that increasing the concentration of Eudragit S100 increased the lag time because it forms a stronger pH-dependent barrier and protects the drug from premature release in the upper gastrointestinal tract. The 3D plot also confirms this increasing trend, with the maximum lag time observed near formulation F7. The drug release contour and 3D surface plot show that the highest drug release at 12 hours was also obtained near F7, which contained an optimized polymer ratio and showed about 3.2 h lag time and 94% drug release. This indicates that F7 provided the best balance between delayed release and complete drug release in colonic conditions. In contrast, formulations with higher Eudragit L100 and ethyl cellulose levels, such as F8 and F9, showed reduced final release because excessive polymer concentration restricted drug diffusion. Therefore, F7 was selected as the optimized batch for colon-targeted Ozanimod delivery.

Fig 7: The DOE contour and 3D surface plots
3.4 Effect of polymers on lag time and drug release
The polymer system strongly influenced lag time and the extent of Ozanimod release. Lag time varied from 1.7 to 3.2 h across the nine formulations, while cumulative drug release at 12 h ranged from 70% to 94%. Formulations containing lower Eudragit S100 concentration showed shorter lag phases and lower release performance. Increasing Eudragit S100 generally improved delayed-release behavior because this polymer dissolves at a higher pH threshold and provides stronger protection against premature release in acidic and early intestinal conditions.
F7, containing 60 mg Eudragit S100, 20 mg Eudragit L100 and 10 mg ethyl cellulose, produced the longest lag time of 3.2 h and the highest 12 h drug release of 94%. This combination appears to provide an optimal balance: Eudragit S100 delays drug release until the target pH region is reached, whereas the moderate amount of Eudragit L100 and lower ethyl cellulose content avoid excessive diffusion resistance. In contrast, F8 and F9 contained higher levels of Eudragit L100 and ethyl cellulose and showed lower release values of 77% and 75%, respectively, indicating that excessive polymer loading restricted drug diffusion.
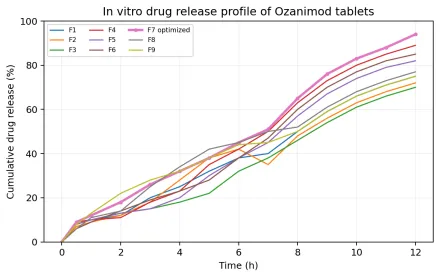
Figure 8. In vitro cumulative release profiles of F1-F9 in sequential dissolution media.
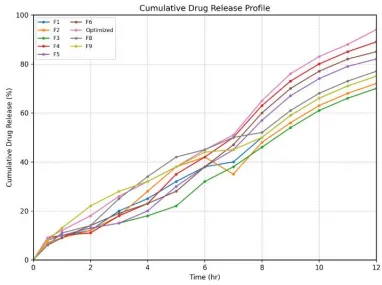
Figure 9. cumulative drug release profile
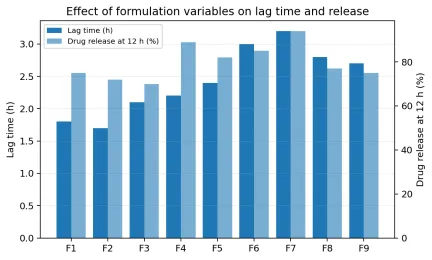
Figure 10. Comparison of lag time and 12 h drug release among factorial batches.
3.5 Factorial design interpretation
The factorial design confirmed that polymer concentration was a critical formulation variable. The lag-time model was statistically significant, and Eudragit S100 was the most influential factor, showing a strong positive effect on lag time. The drug release model also indicated that Eudragit S100 had the dominant contribution to release behavior. The response pattern suggested that adequate Eudragit S100 is required for colon-targeted delay, but excessive combined polymer concentration may decrease the final amount of drug released. Therefore, optimization required balancing pH-dependent protection with sufficient permeability after the lag phase.
3.6 Stability of optimized formulation
The optimized formulation F7 remained physically stable over three months. Appearance remained unchanged, thickness decreased only slightly from 2.5 to 2.4 mm, hardness decreased from 3.3 to 3.1 kg/cm² and friability increased marginally from 0.42% to 0.45%, still below the usual 1% limit. Drug content decreased from 99.6% to 98.5%, cumulative drug release changed from 94% to 93%, and lag time remained nearly unchanged at 3.2- 3.1 h. These findings indicate that the optimized formulation retained its physical, chemical and functional properties during the study period.
Table 6. Stability study of optimized F7 formulation.
|
Parameter |
Initial |
1 month |
2 months |
3 months |
|
Appearance |
White, smooth tablets |
No change |
No change |
No change |
|
Thickness (mm) |
2.5 |
2.5 |
2.5 |
2.4 |
|
Hardness (kg/cm²) |
3.3 |
3.2 |
3.2 |
3.1 |
|
Friability (%) |
0.42 |
0.43 |
0.44 |
0.45 |
|
Weight variation (mg) |
200 |
200 |
199 |
199 |
|
Drug content (%) |
99.6 |
99.2 |
98.9 |
98.5 |
|
Drug release (%) |
94 |
94 |
93 |
93 |
|
Lag time (h) |
3.2 |
3.2 |
3.2 |
3.1 |
CONCLUSION
The study successfully developed and evaluated colon-targeted Ozanimod tablets using Eudragit S100, Eudragit L100 and ethyl cellulose as release-modifying polymers. Preformulation and compatibility studies supported the suitability of the drug and selected excipients for tablet development. The wet granulation method produced tablets with acceptable precompression and post-compression characteristics. Among the prepared formulations, F7 was optimized because it provided the most favorable balance between delayed release and high cumulative drug release, with lag time of 3.2 h, drug content of 99.6% and 94% drug release at 12 h. Stability results indicated that F7 maintained its functional performance for three months. The optimized formulation has promising potential as a colon-targeted oral delivery system for Ozanimod, although in vivo localization, pharmacokinetic performance and therapeutic efficacy should be confirmed in future studies.
FUTURE SCOPE
Future work should include in vivo pharmacokinetic and pharmacodynamic studies to correlate in vitro dissolution with colonic localization and therapeutic performance. Gamma scintigraphy or radiographic tracking may be used to confirm gastrointestinal transit and site of release. Additional long-term stability testing, scale-up trials and Quality by Design-based process optimization are recommended before clinical translation. The formulation platform may also be explored for other drugs requiring site-specific or time dependent delivery to the lower gastrointestinal tract.
ACKNOWLEDGEMENT
The author acknowledges Dr. Vedprakash Patil Pharmacy College, Chhatrapati Sambhajinagar, for academic support and laboratory facilities.
Conflict of Interest
The author declares no conflict of interest.
Funding
No specific funding was declared for this manuscript.
Ethical Approval
Not applicable, as the reported work was an in vitro formulation and evaluation study.
REFERENCES

Achal Patmase*, Dipali Hamde, Formulation and Evaluation of Colon-Targeted Ozanimod Tablets for Inflammatory Bowel Disease Using a Factorial Design Approach, Int. J. Med. Pharm. Sci., 2026, 2 (7), 441-451. https://doi.org/10.5281/zenodo.21272990
 10.5281/zenodo.21272990
10.5281/zenodo.21272990