
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1Pharm D Intern, Ezhuthachan College of Pharmaceutical Sciences, Marayamuttom Neyyattinkara, Thiruvananthapuram.
2Assistant Professor, Department of Pharmacy Practice, Ezhuthachan College of Pharmaceutical Sciences, Marayamuttom, Neyyattinkara, Thiruvananthapuram.
3HOD/Principal, Department of Pharmacy Practice, Ezhuthachan College of Pharmaceutical Sciences, Marayamuttom, Neyyattinkara, Thiruvananthapuram
Left-sided non-occlusive ischemic colitis is an uncommon manifestation of colonic ischemia, typically occurring in the presence of well-established vascular or systemic risk factors. Ischemic colitis commonly affects elderly patients with identifiable vascular or systemic risk factors. however, on-occlusive involvement of the left colon without classical predisposing conditions remains rare. We report a rare case of a 59 years old female who lacked classical predisposing conditions such as atherosclerotic disease, atrial fibrillation or hypotensive episodes. The patient had an past medical history of hypertension, type II diabetes mellitus and hypothyroidism. The patient was presented with more than ten days of left-sided abdominal pain, increased bowel frequency, and intermittent passage of small quantities of stool without hematochezia, had an history of intermittent constipation for six months, altered bowel habits for one week before hospitalization and diagnosis was established through characteristic radiological and endoscopic findings in the absence of mesenteric vessel occlusion. Prompt conservative management led to significant clinical improvement without the need for surgical intervention. This case highlights the importance of maintaining a high index of suspicion for ischemic colitis even in low-risk patients presenting with compatible clinical features.
Ischemic colitis is a form of gastrointestinal ischemia characterized by transient or persistent reduction in blood flow to the colon, resulting in mucosal inflammation, ulceration, and varying degrees of bowel injury. It most commonly affects watershed areas of the colon, particularly the splenic flexure and recto sigmoid junction, and may occur due to occlusive or non-occlusive mechanisms. The severity of ischemic injury ranges from mild, reversible mucosal damage to transmural necrosis requiring surgical intervention. It is the most common type of intestinal ischemia and predominantly affects older adults. Early recognition is essential to prevent progression and complications. Clinical presentation may be subtle and mimic other forms of colitis, leading to diagnostic delay [1].
Occlusive ischemic colitis results from mechanical obstruction of colonic blood vessels, leading to reduced or absent blood flow. The main causes include arterial thrombosis due to atherosclerosis, arterial embolism often originating from atrial fibrillation or cardiac valvular disease, and mesenteric venous thrombosis associated with hypercoagulable states. Other causes include vasculitis, external compression by tumors, and iatrogenic vascular injury following abdominal or vascular surgery. These causes are less common than non-occlusive mechanisms but are typically associated with more severe disease and poorer outcomes [2].
Non-occlusive ischemic colitis occurs due to reduced colonic perfusion without demonstrable vessel blockage, usually from systemic or localized hypoperfusion. Common causes include hypotension, dehydration, shock, heart failure, and sepsis, leading to low-flow states. Medications such as vasoconstrictors, diuretics, NSAIDs, digitalis, oral contraceptives, and chemotherapeutic agents may contribute by reducing blood flow or altering microvascular circulation. Other causes include constipation with increased intraluminal pressure, strenuous exercise, and microvascular dysfunction, particularly in elderly or low-risk patients. This is the most frequent mechanism underlying ischemic colitis [3].
This condition is associated with several risk factors that predispose to reduced colonic blood flow or vascular compromise. Advanced age is the most significant risk factor due to age-related vascular changes and reduced collateral circulation. Hypercoagulable states, smoking, and recent abdominal or vascular surgery further contribute to the risk of developing ischemic colitis [4].
Primarily results from a reduction in blood flow to the colon, leading to insufficient oxygen delivery and subsequent tissue injury. The colon is particularly vulnerable in watershed areas, such as the splenic flexure and rectosigmoid junction, where arterial perfusion is naturally less robust. Ischemia can be occlusive, due to arterial thrombosis, embolism, or atherosclerosis, or non-occlusive, caused by systemic hypoperfusion, hypotension, or vasospasm. Reduced perfusion triggers mucosal and submucosal injury, initially causing edema, ulceration, and hemorrhage, while severe or prolonged ischemia may result in transmural necrosis. Inflammatory mediators and reactive oxygen species exacerbate cellular damage, contributing to local inflammation and bacterial translocation. The degree and duration of ischemia determine the clinical course, ranging from self-limited, transient ischemic colitis to fulminant, gangrenous disease. Chronic ischemia may lead to fibrosis and stricture formation, whereas acute severe injury can precipitate perforation, sepsis, and multiorgan failure. Uiinderstanding the interplay of vascular anatomy, systemic hemodynamics, and colonic susceptibility is key to anticipating disease severity and guiding management [5].
It is classified based on etiology, location, and severity. Etiologically, it is divided into occlusive ischemic colitis (arterial or venous obstruction) and non-occlusive ischemic colitis (hypoperfusion without vessel blockage). Anatomically, it may be left-sided (most common), right-sided, segmental, or pancolonic. Based on severity, ischemic colitis is categorized into transient reversible ischemia, chronic segmental colitis, ischemic stricture, and gangrenous colitis. Acute and chronic forms are recognized, with chronic disease resulting from repeated ischemic insults [6].
Non-occlusive ischemic colitis: Occurs due to transient reduction in colonic blood flow without mechanical obstruction of mesenteric vessels, commonly related to low-flow states or microvascular dysfunction [7].
Occlusive ischemic colitis: Results from arterial or venous obstruction caused by thrombosis, embolism, or external compression, leading to more severe and often extensive colonic ischemia [8].
Left-sided ischemic colitis: The most common form, involving the splenic flexure, descending colon, or sigmoid colon, typically affecting watershed areas with limited collateral circulation [9].
Right-sided ischemic colitis: Involves the cecum and ascending colon and is often associated with severe disease, poorer prognosis, and higher risk of progression to transmural necrosis [10].
Segmental ischemic colitis: Ischemic injury confined to a specific segment of the colon with intervening normal mucosa, often reflecting localized hypoperfusion [11].
Pancolonic ischemic colitis: A rare and severe form involving the entire colon, usually associated with profound hypotension, shock, or systemic hypoperfusion [12].
Transient (reversible) ischemic colitis: A mild form characterized by temporary mucosal ischemia with complete clinical and endoscopic recovery following conservative management [13].
Chronic ischemic colitis: Develops due to repeated or persistent ischemic insults, leading to chronic inflammation, fibrosis, and possible stricture formation [14].
Gangrenous ischemic colitis: The most severe form, marked by transmural infarction, necrosis, and high risk of perforation, requires urgent surgical intervention [15].
Patients with ischemic colitis typically present with sudden onset crampy abdominal pain, most often localized to the left lower quadrant, followed by an urgent desire to defecate. Altered bowel habits such as diarrhea or constipation are common, and many patients experience hematochezia or blood-streaked stools within 24 hours. Systemic symptoms may include low-grade fever, nausea, and vomiting. In mild cases, symptoms may be self-limiting, while severe cases may present with peritonitis, shock, or sepsis. The clinical presentation can vary depending on the extent and severity of ischemia [16]. Complications of ischemic colitis range from mild to life-threatening depending on disease severity and timeliness of intervention. Acute complications include bowel necrosis, perforation, peritonitis, sepsis, and hemorrhage. Chronic complications may involve colonic strictures, chronic ischemic colitis and recurrent episodes of abdominal pain and bleeding. Severe cases may progress to multiorgan dysfunction. Mortality is higher in right-sided and gangrenous ischemic colitis [17]. The diagnosis of ischemic colitis is based on a combination of clinical suspicion, laboratory findings, imaging, and endoscopic evaluation. Laboratory tests may show leukocytosis, elevated inflammatory markers, and metabolic acidosis in severe cases. Contrast-enhanced computed tomography of the abdomen is the imaging modality of choice and may reveal bowel wall thickening, thumb printing and reduced enhancement without vascular occlusion. Colonoscopy is the gold standard for diagnosis, demonstrating edematous, friable mucosa, erythema, erosions, and ulcerations. Biopsy findings support the diagnosis and help exclude infectious or inflammatory bowel disease [18].
Conservative management is appropriate for mild to moderate ischemic colitis without signs of peritonitis or bowel necrosis. Treatment includes bowel rest, intravenous fluid resuscitation, correction of hypotension, electrolyte imbalances and discontinuation of offending medications. Broad-spectrum antibiotics are often administered to prevent bacterial translocation. Pain control and close clinical monitoring are essential. Most patients respond well to conservative therapy with complete clinical and endoscopic recovery [19].
Surgical intervention is indicated in patients with severe ischemic colitis complicated by bowel infarction, perforation, persistent bleeding, or failure of conservative management. Surgical options include segmental colectomy or subtotal colectomy depending on disease extent. Emergency surgery is required in cases of peritonitis or gangrene. Postoperative morbidity and mortality are significant, particularly in elderly patients and those with comorbidities. Early surgical consultation improves outcomes in high-risk cases [20].
Left-sided non-occlusive ischemic colitis without classical risk factors represents a rare and atypical clinical entity characterized by ischemic injury confined to the left colon in the absence of major vascular disease or systemic hypo perfusion. The condition is thought to result from transient microvascular dysfunction or localized hypo perfusion rather than large-vessel obstruction. Clinical presentation may be subtle and mimic other forms of colitis, leading to diagnostic delay. Colonoscopy typically reveals segmental ischemic changes, while imaging excludes mesenteric vessel occlusion. Recognition of this rare presentation is crucial to ensure timely diagnosis and appropriate conservative management [21]. Here we report a case of Left-sided non-occlusive ischemic colitis was confirmed by symptoms and diagnosed through CT scan, colonoscopy, biopsy and effectively managed with conservative therapy.
Case Presentation
A 59 years old female was presented with complaints of more than ten days of left-sided abdominal pain, increased bowel frequency, and intermittent passage of small quantities of stool without hematochezia, had an history of intermittent constipation for six month, altered bowel habits for one week before hospitalization. She had an past medical history of hypothyroidism, hypertension, type II diabetes mellitus and was on medication.
The patient was conscious, oriented, chest clear, air entry bilaterally equal, heart sounds were normal and GIT was soft and left iliac fossa tenderness. During admission the patient had an pulse rate of 80 beats/minute, respiratory rate of 28 breaths/minute, peripheral capillary oxygen saturation was 97% and the blood pressure was 120/90 mmHg.
The patient’s laboratory investigation reports showed an elevation in CRP, HbA1c, polymorphs, carcinoembryonic antigen (CEA) and declined parameters were lymphocytes, serum potassium. The diagnosis was done through USG abdomen and pelvis, CECT scan of abdomen, colonoscopy and biopsy.
USG abdomen and pelvis showed possibilities includes IBD or infective or ischemic colitis, grade I fatty liver. Suggested CECT scan with adequate bowel preparation for further characterization and to rule out malignancy.
CECT scan abdomen and pelvis showed large segments in the circumferential symmetric enhancing bowel wall thickening in sigmoid, descending and left 1/3rd of transverse colon with adjacent fat stranding with pericolic vascular engorgement mild free fluid and few subcentimetric mesenteric lymph nodes and there is no evidence of collection, perforation, large bowel obstruction and the findings are suggestive of inflammatory or infective etiology.
Second time taken CECT scan of abdomen and pelvis showed diffuse circumferential wall thickening in the sigmoid, distal and of transverse colon with wall thickness of approximately 12mm with adjacent fat stranding, hyperemia, pericolic fluid and adjacent lymph nodes and there is no evidence of thrombosis or superior mesenteric vein and its branches. Contrast opacifications noted in the superior mesenteric artery, inferior mesenteric artery and its branches and normal enhancement of bowel wall and no evidence of pneumatosis intestnalis.
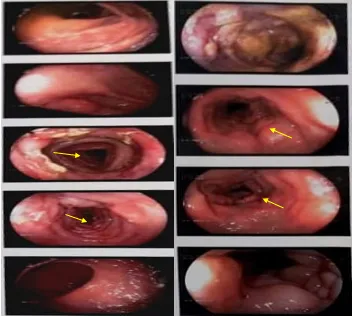
Figure 1: Colonoscopy images: The arrow marks indicates the reduction in the blood flow to the colon ie; ischemic colits
The first colonoscopy revealed two small depressed aphthous-like ulcers in the ascending colon, with surrounding edema, and additional erosions and small ulcers in the transverse colon. The descending and sigmoid colon showed luminal narrowing with edematous mucosa and reduced vascularity, and clean-based depressed ulcers were noted. The rectum and anal canal appeared normal. Biopsies were obtained from multiple sites including the ascending, transverse, descending, and sigmoid colon for further evaluation. These findings were interpreted as colitis, with a possible infectious etiology suggested.
The second colonoscopy revealed multiple ulcers in the descending and sigmoid colon, which appeared larger compared to the previous examination. There was reduced mucosal vascularity noted throughout the affected segments, accompanied by a bluish tinge and luminal narrowing. The distal sigmoid colon and rectum also demonstrated decreased vascularity, while the anal canal appeared normal. Biopsies were taken from the ulcerated areas for further histopathological evaluation. The overall findings were suggestive of an inflammatory bowel disease, with a differential impression of Crohn’s disease.
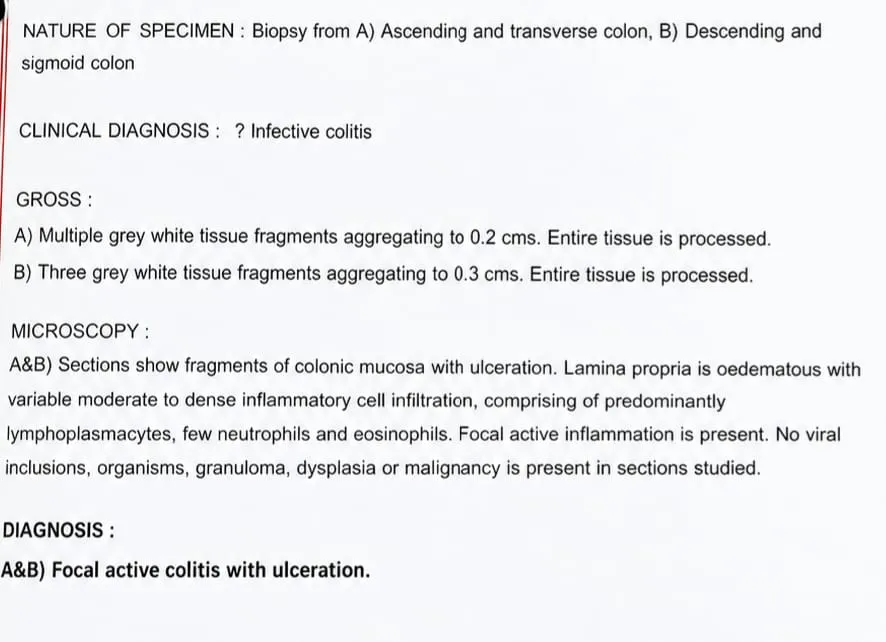
Figure 2: Biopsy Report I
The first biopsy report revealed fragments of colonic mucosa with ulceration and an edematous lamina propria containing a moderate to dense inflammatory infiltrate, predominantly lymphoplasmacytic, with a few neutrophils and eosinophils. The presence of focal active inflammation suggests an acute-on-chronic inflammatory process. Importantly, there is no evidence of viral inclusions, infective organisms, granulomas, dysplasia, or malignancy, which helps exclude infectious colitis, inflammatory bowel disease with granulomatous pattern, and neoplastic pathology. Overall, these features are consistent with focal active colitis with ulceration, a nonspecific pattern that can be seen in transient ischemic, infectious, or drug-related injury.
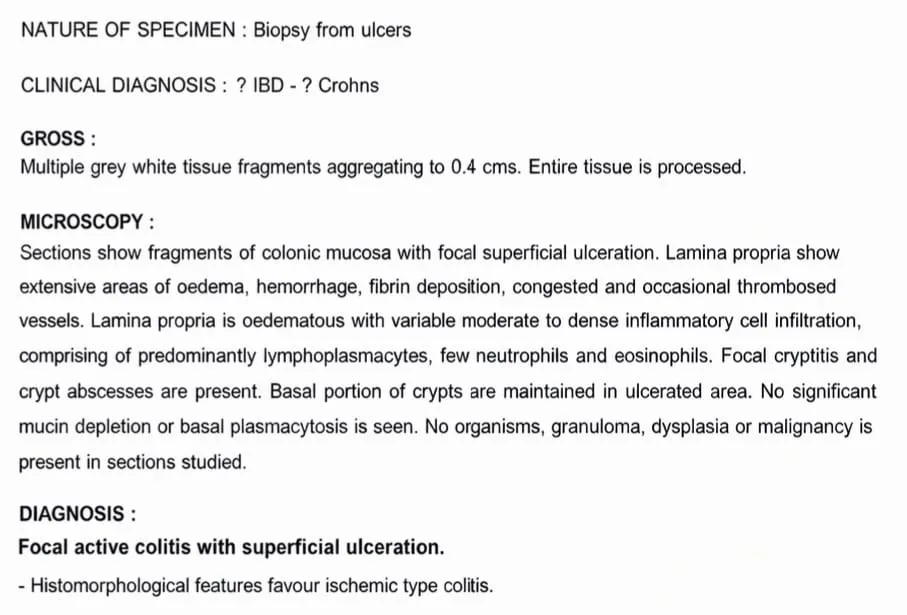
Figure 3: Biopsy Report II
The second biopsy report revealed colonic mucosa with focal superficial ulceration and more prominent lamina propria changes, including extensive edema, hemorrhage, fibrin deposition, vascular congestion, and occasional thrombosed vessels. There is a variable moderate to dense inflammatory infiltrate with lymphoplasmacytes, scattered neutrophils, and eosinophils, along with focal cryptitis and crypt abscesses, while the basal portions of crypts are preserved in ulcerated areas. The absence of significant mucin depletion or basal plasmacytosis, along with negative findings for organisms, granulomas, dysplasia, and malignancy, supports a non–IBD pattern of injury. The overall histomorphological features favors for ischemic-type colitis, correlating with acute mucosal injury due to compromised blood flow rather than chronic inflammatory bowel disease. The patient condition was managed with Inj. Acetylcystiene 1gm IV Q8H and changed to Tab. Acetylcystiene 600 mg P/O BD to treat ischemic colitis as a adjunctive and supportive role by reducing oxidative stress and improving microcirculatory function , Inj. Metronidazole 500 mg IV Q8H to treat infections related to ischemic colitis, INJ.MEROPENEM 1gm IV Q8H to treat infections related to ischemic colitis, INJ.ESOMEPRAZOLE 40 mg IV BD to treat gastric irritation, Inj. Paracetamol 1gm IV BD to relieve pain, TAB. Cyclopam (Dicylcomine Hydrochloride+ Paracetamol 20mg + 500mg P/O BD) to relieve abdominal pain, INJ.TIGEYCYCLINE 50mg IV BD to treat infections related to ischemic colitis, Tab. Mesalamine (5- Amino Salicylic Acid 1.2gm P/O BD) to treat ischemic colitis as adjunctive treatment in mild to moderate cases once acute ischemia has stabilized. Its role is based on its anti-inflammatory action on the colonic mucosa, INJ. CEFOPERAZONE + SULBACTUM 1.5gm IV BD to treat infections related to ischemic colitis, INJ.ONDANSETRON 4mg IV TDS to treat nausea and vomiting, Tab. Remmag (Heavy Magnesium Oxide 400mg P/O BD) to treat constipation, CAP VSL 3 (Streptococcus Thermophilus, Bifidobacterium Longum, Bifidobacterium Breve, Bifidobacterium Infantis, Lactobacillus Acidophilus, Lactobacillus Plantarum, Lactobacillus Paracasei, Lactobacillus Delbrueckii Subsp. Bulgaricus 1 Cap Od To Treat Ischemic Colitis (Adjunctive Therapy During Recovery), Syp. Potklor (POTASSIUM CHLORIDE 20ml P/O TDS to treat hypokalemia, TAB.ASPIRIN 100mg P/O OD to prevent thrombosis, TAB.LEVOTHYROXINE SODIUM 25 mcg P/O OD to treat hypothyroidism, TAB. GLIMEPRIDE+ METFORMIN 1mg + 500mg P/O OD to treat type II diabetes mellitus and Tab. Telmisartan 40mg P/O OD to treat systemic hypertension.
DISCUSSION
Left-sided non-occlusive ischemic colitis without classical risk factors is a rare clinical entity and often poses diagnostic uncertainty. Vakil A et al [22] reported ischemic colitis in a young female without identifiable risk factors who presented with acute abdominal pain and responded well to conservative management; in comparison, our patient was older and had a more subacute presentation with prolonged symptoms, yet similarly lacked major vascular risk factors and showed favorable response to conservative therapy. Lee S O et al [23] described colonoscopy-induced ischemic colitis in patients without predisposing conditions, highlighting iatrogenic hypoperfusion as a trigger, whereas our case occurred spontaneously without procedural or external precipitating factors, suggesting an idiopathic low-flow mechanism. Al Mohannadi F et al [24] involved a middle-aged woman in whom ischemic colitis mimicked inflammatory bowel disease, leading to diagnostic delay; similarly, our patient presented with nonspecific symptoms and altered bowel habits, emphasizing the overlapping clinical features and diagnostic challenge in low-risk individuals. Lee J H et al [25] demonstrated a mass-forming variant of ischemic colitis without vascular disease, representing an atypical morphological presentation, while our case showed classical ischemic changes confined to the left colon without mass formation, reinforcing the heterogeneity of disease patterns. Shi J et al [26] reported ischemic colitis in a patient without significant comorbidities but with severe mucosal injury, whereas our patient had a milder, non-gangrenous form that responded well to conservative management. Compared with these reported cases, our case highlights that left-sided non-occlusive ischemic colitis can present insidiously in patients without classical risk factors and can be successfully managed conservatively when diagnosed early.
Clinical Significance
This case underscores the importance of recognizing ischemic colitis as a potential diagnosis even in patients who lack classical vascular or systemic risk factors. Left-sided non-occlusive ischemic colitis without identifiable precipitating factors is rare and may easily be misdiagnosed as infectious or inflammatory colitis. Early consideration of ischemic colitis in low-risk patients presenting with persistent abdominal pain and altered bowel habits facilitates timely diagnostic evaluation. Characteristic radiological and endoscopic findings play a crucial role in establishing the diagnosis in such atypical presentations. Prompt diagnosis allows for appropriate conservative management and prevents progression to severe complications. This case highlights the need for heightened clinical awareness to avoid diagnostic delay.
THERAPEAUTIC CHALLENGES
The management of non-occlusive ischemic colitis without classical risk factors poses several therapeutic challenges. The absence of typical predisposing conditions may delay diagnosis and initiation of appropriate treatment. Differentiating ischemic colitis from inflammatory bowel disease or malignancy is often difficult, particularly when endoscopic findings overlap. Decisions regarding the use of antibiotics, anti-inflammatory agents, and supportive therapies must be individualized due to limited evidence-based guidelines. Close clinical monitoring is essential to detect disease progression or complications requiring surgical intervention. Conservative management requires careful balancing of bowel rest, hydration, and symptom control to ensure favorable outcomes.
CONCLUSION
Left-sided non-occlusive ischemic colitis without classical risk factors represents a rare and diagnostically challenging clinical entity. This case demonstrates that ischemic colitis can occur in patients without significant vascular disease or hemodynamic compromise. A high index of suspicion, combined with timely imaging and endoscopic evaluation, is critical for accurate diagnosis. Conservative management can be effective when instituted early in clinically stable patients. Awareness of such atypical presentations is essential to prevent unnecessary surgical interventions. Reporting rare cases such as this contributes to improved understanding and clinical recognition of non-occlusive ischemic colitis.
REFERENCES


Ardra S. A.*, Grace N. Raju, Shaiju S. Dharan, Left- Sided Non-Occlusive Ischemic Colitis Without Classical Risk Factors: A Rare Clinical Entity, Int. J. Med. Pharm. Sci., 2026, 2 (6), 439-446. https://doi.org/10.5281/zenodo.21037852
 10.5281/zenodo.21037852
10.5281/zenodo.21037852