
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
School of Pharmaceutical Sciences, Lovely Professional University, Phagwara (Punjab), India
Background: Metabolic dysfunction-associated steatotic liver disease (MASLD) represents the most prevalent chronic liver condition globally, affecting approximately 32% of the adult population and imposing a substantial burden of morbidity and healthcare expenditure. The progressive spectrum of MASLD encompassing simple hepatic steatosis, metabolic dysfunction-associated steatohepatitis (MASH), fibrosis, cirrhosis, and hepatocellular carcinoma currently lacks approved pharmacological treatments targeting the foundational pathogenic mechanisms. Central to MASLD pathogenesis is the gut-liver axis, a bidirectional communication network linking intestinal microbial ecology with hepatic metabolic and immunological functions through the portal venous circulation, bile acid signaling, and microbial metabolite trafficking. Objective: The present review gives a comprehensive insight into the pathophysiology of gut-liver axis disorder associated with MASLD and explores the therapeutic potential of plants in the regulation of these disease processes through gut dysbiosis, increased gut permeability, LPS-TLR4 pathways, bile acid metabolism, oxidative stress, and inflammation-related cytokine pathways. Methods: The search strategy included the use of key terms and MeSH terms such as MASLD, NAFLD, gut-liver axis, gut microbiota, herbal medicine, curcumin, berberine, silymarin, EGCG, resveratrol, and quercetin in the PubMed, Scopus, Web of Science, and Google Scholar online databases. Preclinical studies, randomized control trials, systematic reviews, and systems biology studies from 2000 to 2024 were included in the review. Results: Gut dysbiosis in MASLD patients is defined by an abnormal rise in the ratio between Firmicutes and Bacteroidetes bacteria, loss of beneficial bacteria such as Akkermansia muciniphila, Bifidobacterium, and Faecalibacterium prausnitzii, and an excessive amount of enteric bacteria that produce lipopolysaccharides such as Enterobacteriaceae. Such disturbances affect the intestinal epithelium, causing an increased permeability of endotoxins, entering the portal vein to trigger inflammation through hepatic Kupffer cells and TLR4-NF-κB pathways. In turn, this process leads to steatohepatitis, insulin resistance, oxidative stress, and eventually fibrosis. Natural products like curcumin, berberine, EGCG, silymarin, resveratrol, and quercetin exhibit multiple targets of action on this pathway by acting on FXR, TGR5, AMPK, Nrf2, SIRT1, and PPAR-alpha signaling pathways. Conclusions: Herbal medicines targeting the gut–liver axis represent a scientifically grounded, multi-mechanistic therapeutic strategy for MASLD. Integration of metagenomics, metabolomics, and network pharmacology approaches is essential to optimize phytochemical-based interventions and accelerate their translation into clinical practice. Long-term safety data, strong clinical trial designs, and standardization of bioactive extracts continue to be top priorities.
Metabolic dysfunction-associated steatotic liver disease (MASLD), formerly known as non-alcoholic fatty liver disease (NAFLD) until a new name was agreed upon globally, has become the most prevalent chronic liver disease worldwide, accounting for 32.4% of global cases and increasing as a result of the ongoing epidemics of obesity, type 2 diabetes mellitus (T2DM), and metabolic syndrome [1, 2]. The Delphi consensus panel of key hepatology societies adopted the new MASLD terminology in 2020 in order to capture the underlying metabolism and avoid the stigmatizing term of ‘non-alcoholic’ [3]. MASLD is predicted to become the main reason for liver transplantations over the next two decades in developed countries surpassing viral hepatitis [4, 5]. This disorder does not affect only wealthy nations; according to systematic meta-analysis that involved 86 studies and more than 8.5 million people from 22 countries, the worldwide prevalence of the disease exceeded 25%, while the highest rates were noted in the Middle East (32%), South America (31%), and Asia (27%) [1]. For example, in South Asia (including India), there is another special phenotype associated with MASLD called ‘lean MASLD,’ in which the condition affects patients without obesity but characterized by significant fibrosis, as measured by normal body mass index [5]. The economic impact of MASLD on society is considerable, with the USA experiencing more than $103 billion annually in terms of its cost burden [4].
MASLD is a spectrum of pathological conditions starting from uncomplicated fatty liver disease, which is described as an excess lipid accumulation more than 5% of hepatocytes, progressing through metabolic dysfunction associated steatohepatitis (MASH), which has features such as hepatocyte ballooning, lobular inflammation, and various stages of fibrosis [6]. Around 15-25% of cases with uncomplicated fatty liver disease progress to MASH, and out of those, 10-25% of individuals develop cirrhosis after ten years. The traditional two-hit theory postulated by Day and James, where the first hit refers to steatosis, and the second hit is oxidative stress or inflammatory factors, has been replaced by the multiple parallel hits model, which includes gut dysbiosis, adipokine imbalance, endoplasmic reticulum stress, and mitochondrial impairment [7, 8]. The development of cirrhosis is the decisive threshold stage, beyond which the patient will have significant morbidity of portal hypertension, decompensated liver disease, and hepatocellular carcinoma (HCC). The incidence of HCC in MASH-related cirrhosis has an estimated annual rate of 2-4%, equivalent to HCC occurrence rates in hepatitis C cirrhosis [9, 10]. The daunting statistics highlight the necessity of developing innovative medications that address the basic pathological mechanisms of the disease.
Despite numerous investigations conducted in the last few decades, there is currently no specific FDA-approved therapeutic drug for the treatment of MASLD and MASH; therefore, it is an unmet medical need. In terms of lifestyle change therapy, which includes calorie restriction, regular aerobic exercise, and dietary changes, it results in substantial hepatic fat reduction and histological improvement among some dedicated patients, but maintenance is difficult [9]. Clinical trials of pharmacological therapy for MASH have evaluated a variety of agents, including vitamins such as vitamin E (antioxidants), metformin, thiazolidinediones, GLP-1 receptor agonists, FXR agonists, and antifibrotics, with inconsistent and weak effects. Resmetirom was approved in 2024 by FDA for the treatment of MASH patients who have moderate-to-advanced stage liver fibrosis as a significant achievement, though its high cost and unclear mechanism make more work necessary [11]. It should be mentioned that traditional medicinal systems, such as Ayurveda, Traditional Chinese Medicine (TCM), and Unani medicine, have drawn much attention regarding herb-based treatment. These phytochemical drugs inherently have a multifunctional pharmacological profile suitable for the treatment of MASLD because of its pathogenesis. Also, they benefit due to their safety, low cost, and chemical diversity.
The gut-liver axis, a two-way interaction between the intestinal microbiota and the liver through the portal venous circulation, bile acids, cytokines, and microbial metabolites, has become one of the most important pathogenic factors in MASLD [11, 12]. The dysfunction of the axis, which includes microbial dysbiosis, disrupted intestinal barrier integrity, altered bile acid metabolism, and endotoxin-mediated liver inflammation, results in a feedback loop that causes steatosis, sterile hepatitis, and fibrosis [13]. The effects that herbal medicine exerts on the gut liver axis happen simultaneously, hence making their treatment profile ideal for the complexities of MASLD. This review aims to provide an interdisciplinary perspective on the gut-liver axis through the analysis of herbal drugs against MASLD from a mechanistic, clinical, and systems biology standpoint [14].
The basis for the gut-liver axis is the portal system through which all nutrient-rich venous blood from the intestines flows straight into the sinusoidal system of the liver before joining the systemic circulation [15]. The anatomic positioning ensures that the liver is the first immunologic and metabolic filter for whatever the intestinal microbiome produces, allowing contact of hepatocytes, hepatic stellate cells, and Kupffer cells with constant exposure to antigens of bacteria, SCFA, bile acids, and endotoxins such as LPS [16]. However, normal intestinal epithelium with its components, mucus layer, tight junctions between the epithelial cells and the immunocompetent cells in the lamina propria usually prevent luminal contents from moving via the paracellular route into portal circulation [16]. On the other hand, the liver controls the composition of the intestinal environment by bile secretion and IgA production and release of other hepatically produced mediators that affect intestinal permeability and microflora [17].
The integrity of intestinal epithelia is sustained through multiprotein complexes that comprise the tight junctions between adjacent enterocytes. The principal elements comprising these complexes include claudins 1, 3, occludin, and zonula occludens-1, with levels of expression and phosphorylation being indicative of paracellular permeability [16]. A range of mechanisms lead to impairment of the tight junction in MASLDs including high-fat diet patterns, microbial dysbiosis and associated mucolytic enzymes and proteases, LPS elevations activating TLR4 receptors on enterocytes, and SCFA insufficiency limiting epithelial energy supplies [18].
In an important study conducted by Miele et al., a significant increase in intestinal permeability in NAFLD patients was reported compared to control individuals based on lactulose-to-mannitol ratio assessment, where permeability positively correlated with disease severity but negatively with tight junction protein expression [19]. The following studies indicated higher intestinal permeability during all stages of MASLD, from the onset of steatosis, MASH to fibrosis, acting as an etiological factor and disease marker at each stage [20].
Bile acids derived from cholesterol metabolism in the liver perform two roles, one as lipid solubilizers or detergents and the other as signaling agents acting via specific nuclear and membrane receptors [21]. The primary bile acids, cholic acid (CA) and chenodeoxycholic acid (CDCA), undergo conjugation with glycine or taurine in the liver, resulting in their secretion into bile. Once in the colon, the bile acids undergo deconjugation and conversion by gut bacteria to secondary bile acids, deoxycholic acid (DCA), and lithocholic acid (LCA). The farnesoid X receptor (FXR, NR1H4), a member of the nuclear receptor family and highly abundant in hepatocytes and enterocytes, acts as the bile acid receptor to modulate a transcriptional program responsible for reducing bile acid production through SHP and FGF19, decreasing lipid production through downregulation of SREBP-1c, increasing fatty acid β-oxidation, and protecting the intestinal barrier [22]. The G-protein coupled receptor TGR5 (GPBAR1), expressed in enteroendocrine L cells, Kupffer cells, and brown adipose tissue, activates upon stimulation by secondary bile acids and increases GLP-1 secretion by L cells, increases thyroid hormone activation in brown adipose tissue, and inhibits the inflammatory response in the liver and macrophages. In MASLD, FXR activity is inhibited globally due to changes in bile acid pool composition caused by dysbiosis [23].
The hepatic immune cell compartment is particularly characterized with having a unique architecture that helps to maintain tolerance for dietary antigens and microbial antigens derived from commensal bacteria while being capable of defending against real threats posed by pathogens. Kupffer cells, which are resident liver macrophages constituting around 30% of the total number of liver non-parenchymal cells, express all major pattern recognition receptors (PRRs) including Toll-like receptors 2, 4, and 9, as well as NOD-like receptors, and are thus able to quickly detect and react to pathogen-associated molecular patterns (PAMPs) translocated from the disbiotic gut [23]. Apart from immune-metabolic communication, there is metabolic communication between the two organs as well. Short-chain fatty acids (SCFAs) that are derived from the microbial fermentation of dietary fiber (primarily acetate, propionate, and butyrate) provide energy, act as epigenetic regulators and signaling molecules through GPR41, GPR43, and GPR109a receptors expressed on colonocytes, immune cells, and hepatocytes. The gut microbiome also affects host energy homeostasis via Fiaf which regulates lipoprotein lipase activity and triglyceride accumulation in adipose tissue [24].
The gut microbiome of humans contains about 1013 organisms with more than 1,000 different species. Of these, two major phyla are Firmicutes and Bacteroidetes, which make up almost all the bacterial phyla in a healthy individual [23]. In MASLD, there is always a decrease in alpha diversity, along with specific changes in the composition at various taxonomical levels [12, 25]. One of the consistent observations across several independent cohorts is the increase in the ratio between Firmicutes and Bacteroidetes. This phenomenon results from an increase in the energy harvesting capability of Firmicutes bacteria that can harvest additional energy from indigestible carbohydrates. At the genus and species level, the hallmarks of MASLD include the depletion of commensals such as Akkermansia muciniphila the Gram-negative bacteria responsible for mucin degradation and maintaining mucosal integrity and metabolic homeostasis in the intestines, Bifidobacterium strains capable of lactate production and deactivating lipopolysaccharides by means of short-chain acids, and Faecalibacterium prausnitzii, the predominant producer of butyrate in the human colon [26]. In contrast, there is an enrichment of pathogenic bacteria like Ruminococcus spp. With high permeability in the intestines, Clostridiales species with increased capacity for secondary bile acid production and ethanol synthesis, and E. coli strains that can produce endotoxins and cause liver inflammation [27]. The study by Boursier et al. showed the existence of characteristic metagenomes in NAFLD patients in relation to histological damage with Ruminococcus enrichment being specific for NASH while Bacteroides enrichment was indicative of progressive fibrosis [28]. Metagenomic analysis performed by Loomba et al. enabled to establish the presence of a gut microbiome signature associated with advanced stages of fibrosis (F3-F4) with an AUROC of 0.87 [29].
Table 1. Gut Microbiota Compositional Changes in MASLD and Their Functional Significance
|
Microbial Taxon |
Change in MASLD |
Functional Role |
Key Metabolites |
Clinical Significance |
|
Firmicutes |
Increased |
Energy harvest, SCFA production |
Butyrate, acetate |
Promotes lipogenesis, weight gain |
|
Bacteroidetes |
Decreased |
Polysaccharide fermentation |
Propionate, acetate |
Reduced anti-inflammatory SCFA |
|
Akkermansia muciniphila |
Decreased |
Mucin layer maintenance |
Short-chain fatty acids |
Impaired gut barrier integrity |
|
Bifidobacterium spp. |
Decreased |
Lactate, SCFA production |
Lactate, acetate |
Reduced LPS neutralization |
|
Ruminococcus spp. |
Increased |
Cellulose fermentation |
Hydrogen, formate |
Increased hepatic fat load |
|
Faecalibacterium prausnitzii |
Decreased |
Butyrate, anti-inflammatory |
Butyrate |
Loss of mucosal protection |
|
Clostridiales spp. |
Increased |
Bile acid deconjugation |
Secondary bile acids |
Dysregulated FXR/TGR5 signaling |
|
Escherichia coli |
Increased |
Endotoxin production |
LPS, ethanol |
TLR4-mediated hepatic inflammation |
Table 1: Characteristic alterations in gut microbial composition observed in MASLD patients, with associated functional roles and clinical implications.
Enhanced intestinal permeability, known popularly as the ‘leaky gut’ syndrome, is an essential factor that bridges the relationship between dysbiosis and liver damage in MASLD. Numerous factors such as microbiological elements and dietary choices contribute to increased permeability of the intestinal barrier [30]. Pathogenic bacteria generate zonulin-inducing peptides, claudin-degrading enzymes, and reactive oxygen species, which damage the tight junction proteins [16]. The lack of butyrate production, due to the reduction in the numbers of Faecalibacterium prausnitzii and Bifidobacterium, robs the colonocytes of their main fuel supply, leading to poor function of the epithelial barrier and apoptosis of enterocytes [31]. Besides, high-fat diet alone disrupts the tight junction proteins through the activation of TLR4 and PKCzeta signaling pathways in enterocytes [32]. Consequently, impaired paracellular permeability allows microbial products such as LPS, peptidoglycan, bacterial DNA (CpG oligodeoxynucleotides), and living bacteria to be transferred to the mesenteric lymphatics and portal circulation, hence exposing the liver immune system to a continuous endotoxin load [33]. This mechanism is supported by increased serum levels of LBP, antibodies against LPS, and sCD14 found in MASLD patients as opposed to healthy individuals [20].
Lipopolysaccharides (LPSs), which make up the main components of Gram-negative bacterial membranes, are regarded as the typical danger signals that instigate the portal or systemic inflammatory reactions of MASLD [20, 21]. Under normal circumstances, minimal amounts of LPS are constantly transported into the portal circulation, but they can be easily removed by Kupffer cells from the liver without provoking an inflammatory reaction [22]. On the contrary, in MASLD, LPS entry into the bloodstream is greatly increased by the increased permeability of the intestine along with the development of a dysbiotic colonization of LPS-producing Enterobacteriaceae. LPS binds selectively to MD-2/TLR4 complexes that are highly expressed on the surfaces of Kupffer cells, hepatocytes, and hepatic stellate cells. Further signaling involves either MyD88-dependent or TRIF-dependent signaling pathways leading to activation of NF-κB and IRF3, respectively. NF-κB activation triggers the transcription of many inflammatory mediators, such as TNF-alpha, IL-1beta, IL-6, IL-12, and COX-2, thus forming a positive feedback loop for liver inflammation [34].
Insulin resistance is a consequence of MASLD via several convergent pathways involving gut dysbiosis. Gut dysbiosis causes an increase in circulating LPS, which activates TLR4-mediated signaling in adipocytes and skeletal muscles. This results in serine phosphorylation of IRS-1 mediated by the IKK-beta and JNK pathways, leading to disruption of insulin-mediated signaling [20]. Also, dysbiosis influences the function of the incretin hormone system by causing a decrease in GLP-1 production by L-cells owing to changes in bile acids and reduced activation of TGR5 receptor [35]. In the liver, insulin resistance impairs the regulation of synthesis and export of lipids by increasing de novo lipogenesis through SREBP-1c activation while simultaneously disrupting mitochondrial beta-oxidation of fatty acids and VLDL secretion, resulting in fatty acid accumulation [36]. Consequently, increased fatty acid content leads to a pro-inflammatory state in the hepatocytes, predisposing them to inflammation and apoptosis, the pathogenic substrates for MASH.
The major metabolites generated by anaerobic fermentation of dietary fiber and resistant starches in the colon are the short-chain fatty acids acetate (C2), propionate (C3), and butyrate (C4), whose combined daily production rate in healthy individuals is 500-600 mmol [37]. Butyrate acts as an energy substrate for colonocytes (accounting for approximately 70% of colonocyte needs), increases mucus secretion, enhances development of regulatory T cells in the colon lamina propria, and inhibits HDACs, hence producing anti-inflammatory epigenetic changes. Propionate is absorbed from the colon into the portal circulation and exerts anticholesterolemic, antigluconeogenic, and hunger-suppressing effects [38]. Decreased ingestion of dietary fibers and the loss of bacteria involved in SCFAs production (Bifidobacterium, Faecalibacterium prausnitzii, Roseburia) in patients with MASLD result in a sharp decrease in SCFA concentration in the colon lumen. This leads to reduced colonocyte energy supply, decreased mucus secretion, lowered immune regulatory activity, as well as insufficient activity of GPR41/43 receptors needed to inhibit lipogenesis and stimulate GLP-1 release [39]. Therefore, replenishment of SCFA production through prebiotics or probiotics seems a plausible intervention approach.
There is substantial evidence demonstrating qualitative and quantitative remodeling of the bile acid pool, which severely perturbs gut-liver axis homeostasis in MASLD. In MASLD patients, serum bile acids are at higher levels due to their impaired hepatic clearance owing to cholestasis and disruption in the enterohepatic bile acid circulation. The bile acid pool, however, has become increasingly cytotoxic with decreased conjugation efficiency of primary bile acids, and secondary bile acids, in particular, deoxycholic acid (DCA) and lithocholic acid (LCA) are accumulating [40, 41]. Down-regulation of FXR activity leads to numerous metabolic impairments. Lack of inhibition of CYP7A1 by FXR contributes to the excessive bile acid synthesis, whereas down-regulation of FGF19 (FGF21 in rodents) from enterocytes, which normally inhibits CYP7A1 and stimulates fatty acid oxidation in the liver, worsens the already disrupted lipid metabolism in MASLD. Furthermore, FXR regulates immunological responses by inducing IgA synthesis in plasma cells and promoting defensin secretion from Paneth cells; therefore, the down-regulation of FXR results in intestinal immune deficiency in MASLD [41]. Activation of the G protein-coupled bile acid receptor TGR5 by bile acids released in enteroendocrine cells (L cells) promotes the release of GLP-1 and PYY hormones. GLP-1 helps in appetite suppression, enhances insulin sensitization, and inhibits glucagon secretion from alpha cells of the pancreas. TGR5 in brown fat tissues activates the conversion of thyroid hormones in the cell from T4 to T3 mediated by type 2 deiodinase. Therefore, modulation of TGR5 by pharmacological agents is beneficial. Some natural herbs can activate TGR5, including berberine, curcumin, and Ginsenoside Rb1 [42].
The TLR4 signaling pathway acts as the molecular route by which LPS from the gut mediates liver inflammation in MASLD. TLR4 is a class of type I transmembrane glycoprotein that belongs to the pattern recognition receptors group, being the major receptor for LPS from Gram-negative bacteria through its co-receptor complex consisting of MD-2 and CD14. On LPS binding, TLR4 undergoes conformational changes and dimerization to recruit intracellular adaptor proteins, namely MyD88 and TRIF, via their TIR domains [43]. In the MyD88-dependent signaling pathway, LPS-induced activation of IRAK4 and IRAK1 kinases leads to TRAF6 ubiquitination and TAK1 phosphorylation of IKK-beta. Phosphorylated IKK-beta targets IkappaBalpha for proteosomal degradation, thereby releasing NF-kappaB dimers (mainly p65/p50) to enter the nucleus and initiate the transcription of inflammatory genes (> 200). At the same time, MAP kinase pathways activate AP-1 and C/EBP-beta transcription factors through JNK and p38 MAPK pathways, respectively, to increase transcriptional activity further. Hepatic inflammation triggered by TLR4 signaling in MASLD is reinforced by the abundant expression of TLR4 on Kupffer cells and continuous exposure to portal LPS flow from the microbiome-disturbed gut [44].
Oxidative stress, described as an imbalance between ROS production and its detoxification, plays a crucial role in the development and progression of MASLD, as well as liver cell injury [10]. In MASLD, ROS generation may take place through diverse pathways, including electron leak from the mitochondria during fatty acid beta-oxidation, cyclo-oxygenase enzyme (CYP2E1 and CYP4A) cycling activity, NADPH oxidase enzymes (NOX2 and NOX4) activation through the LPS-TLR4 signaling pathway in Kupffer cells, and xanthine oxidase activation [45]. The excess ROS generated in MASLD exceed the body's intrinsic antioxidant protection mechanism (superoxide dismutase, catalase, glutathione peroxidase, and the Nrf2-ARE transcription pathway), causing lipid, protein, and mitochondrial DNA oxidation.
Effects of oxidative stress on mitochondria in MASLD include impaired beta-oxidation efficiency, dysfunction of electron transport chain complexes I and III, poor ATP production, mitochondrial membrane depolarization, and increased mPTP permeability leading to apoptosis and necroptosis of hepatocytes [46]. Oxidative stress-induced lipid peroxidation produces reactive aldehydes (4-HNE and MDA), which form protein-DNA adducts, induce hepatic stellate cell activation via TGF-beta1 signaling, and stimulate fibrogenesis [47].
In MASH, TNF-alpha represents the most crucial component of the cytokine network involved in triggering an inflammatory cascade within the liver [10, 21]. Secreted by Kupffer cells following exposure to LPS-TLR4 ligands, TNF-alpha triggers apoptosis of liver cells via caspase-8 activation via TNFR1 and mitochondria-mediated release of cytochrome c, and also upregulates NF-kappaB-mediated inflammatory gene expression in a positive feedback cycle. MASH patients display higher serum TNF-alpha levels than patients with simple steatosis, and higher expression of TNF-alpha mRNA in the liver correlates with the degree of histological liver damage [48].
Activated Kupffer cells and hepatic stellate cells release IL-6, activating the JAK/STAT pathway and the synthesis of acute phase proteins and impairing insulin signaling due to induction of SOCS3 that decreases insulin receptor substrate phosphorylation. In turn, insulin resistance and the persistence of the lipogenic environment develop as a result [49]. IL-1beta generated by the NLRP3 inflammasome from cholesterol crystals, palmitate, and ATP, contributes to hepatocyte cell death via pyroptosis and also stimulates stellate cell activation and fibrosis [21].
The natural medicine arsenal is endowed with a wide array of phytochemicals with implications for the disease process. In the subsequent subsections, the best understood medicinal herbs that have demonstrated influence on the gut-liver axis are explored based on their mechanisms of action regarding microbiome modulation and hepatoprotection.
Table 2. Herbal Compounds Modulating the Gut–Liver Axis in MASLD: Mechanisms and Evidence Summary
|
Compound |
Source Herb |
Gut Microbiome Effect |
Molecular Target |
Pathway Modulated |
Evidence Level |
|
Curcumin |
Curcuma longa |
Increases Lactobacillus, Bifidobacterium; reduces Firmicutes/Bacteroidetes ratio |
NF-κB, Nrf2, FXR |
Inflammatory cytokines, oxidative stress, bile acid |
Preclinical + Phase II RCT |
|
EGCG |
Camellia sinensis |
Increases Akkermansia, Bacteroidetes; reduces Clostridiales |
AMPK, PPAR-α, TLR4 |
Lipid oxidation, insulin signaling, inflammation |
Preclinical + human observational |
|
Berberine |
Berberis spp. |
Reduces Firmicutes; increases Bacteroidetes, Akkermansia |
AMPK, FXR, TGR5 |
Glucose/lipid metabolism, bile acid |
Phase II–III RCTs |
|
Silymarin |
Silybum marianum |
Modulates Lactobacillus/Clostridium balance |
NF-κB, TGF-β1, Nrf2 |
Fibrosis, oxidative stress, inflammation |
Multiple RCTs |
|
Resveratrol |
Polygonum cuspidatum |
Increases Lactobacillus, Akkermansia |
SIRT1, NF-κB, AMPK |
Lipid biosynthesis, mitochondrial function |
Phase I–II RCTs |
|
Quercetin |
Allium cepa, Capers |
Increases Bifidobacterium; reduces LPS producers |
PI3K/Akt, Nrf2, PPAR-γ |
Oxidative stress, insulin resistance |
Preclinical; limited human data |
|
Ginsenoside Rb1 |
Panax ginseng |
Reverses dysbiosis; increases SCFAs |
FXR, TGR5, AMPK |
Bile acid, glucose metabolism |
Preclinical |
|
Baicalin |
Scutellaria baicalensis |
Reduces Clostridiales; increases Bacteroidetes |
TLR4, NF-κB, Nrf2 |
LPS-mediated inflammation |
Preclinical |
Table 2: Integrated overview of phytochemical regulators affecting gut microbial composition and hepatic signaling pathways in MASLD.
Curcumin has been shown to have multifunctional regulation in pathways of inflammation, oxidation, metabolism, and microbiota-related signaling concerning the development of MASLDs. Curcumin is a fragrant root, which has been traditionally used for culinary and medicinal purposes in South Asia for more than 4,000 years. The mechanism of curcumin works in relation to pleotropic effects, such as ant inflammatory, antioxidant, hypolipidemic, and microbiota modulation via several biological targets [43-47].
Inhibitory effects of curcumin on inflammatory pathways mainly occur through inhibition of NF-κB related pathways but also involve activation of antioxidative stress mechanisms like activation of Nrf2 pathway [49]. It has been suggested that the impact of curcumin-induced changes in gut microbiota enhances intestinal barrier function and leads to reduction in endotoxin-mediated liver inflammation. In this context, curcumin increased the population of Lactobacillus and Bifidobacterium, balanced Firmicutes-to-Bacteroidetes ratio, and decreased the number of Enterobacteriaceae bacteria producing LPS [47, 48]. These changes in microbiota composition were accompanied by increased concentrations of SCFAs in feces, up-regulation of tight junction proteins (ZO-1, claudin-1, occludin), and reduced levels of LPS and LBP in the serum [49-51]. From the point of action mechanism, curcumin is able to inhibit formation of the complex of TLR4-MD2 and activate NF-кappaB signaling in Kupffer cells [52]. As documented in two double-blind, randomized studies conducted by Rahmani et al. and Panahi et al. (both involving administration of 1 g/day phytosomal preparation), there have been statistically significant declines in hepatic fat fraction (MRI-PDFF), ALT, and AST with improvements in liver function profile as well as decreased ALT and AST levels among individuals with NAFLD through phytosome curcumin therapy. Oral bioavailability continues to be an issue that needs to be addressed [53].
Green tea (Camellia sinensis) is one of the most frequently consumed herbal beverages, containing a rich polyphenol profile comprising mainly of catechins, in which epigallocatechin-3-gallate (EGCG) constitutes about 50-80% of total catechin content [50-52]. The use of EGCG to treat metabolic diseases as well as prevent liver damage has been widely studied in various preclinical and clinical studies [52-56]. Metabolic regulation by EGCG is mediated mainly by the role of AMPK in suppression of lipogenesis and induction of fat oxidation in the liver [53, 56]. Moreover, EGCG affects bile acid metabolism through FXR activation and repression of CYP7A1. [56] In the anti-inflammatory action, EGCG was found to suppress the activity of TLR4 receptors, NF-kappaB and NLRP3 inflammasome [52, 55]. Regarding microbiome modulation, there is an increase in the population of Akkermansia muciniphila and Bacteroidetes along with a decrease in the populations of Clostridiales and Firmicutes among mice fed on high-fat diets, along with restored expression of tight junction proteins in the colon and reduction in portal lipopolysaccharides (LPS) [56]. Moreover, the growth of LPS producing Gram negative bacteria is inhibited directly by EGCG, through membrane damage and inhibition of bacterial nucleic acid synthesis [55, 56]. Anti-fibrotic effects of EGCG involve direct inhibition of stellate cell proliferation and transformation via inhibition of TGF-beta1 and SMAD2/3 signaling with reduced expression of alpha-SMA [52]. Pilot randomized controlled trials involving Sakata et al. found significant reductions in levels of serum ALT, AST, and TNF-alpha concentration and a reduction in hepatic echogenicity verified via ultrasound following administration of green tea extract for 12 weeks in 45 patients [54]. Bioavailability of EGCG is hampered due to its intestinal and hepatic metabolism and co-ingestion of milk leads to decreased bioavailability by formation of non-absorptive complexes [51].
Berberine (BBR) is an isoquinoline alkaloid found in many plant species such as Berberis vulgaris (barberry), Berberis aristata (tree turmeric), Hydrastis canadensis (goldenseal), and Coptis chinensis (Chinese goldthread). Berberine is among the phytochemicals that have been most studied as therapeutic agents against metabolic liver disorders. The effectiveness of this natural compound as a therapy is based on several randomized controlled clinical trials [57-61]. The major biochemical effect of berberine as an agent against metabolic disorders includes the activation of AMPK through dual mechanisms of action: mitochondrial respiratory chain complex I inhibition and allosteric AMPK activation (decreasing ATP/AMP ratio and AMPK activation through LKB1) [57]. The AMPK activation by berberine leads to the complete normalization of lipid metabolism, inhibition of de novo lipogenesis by SREBP-1c suppression, decreased FAS and ACC expression, and increased fatty acid beta-oxidation under the control of PPAR alpha [57-60]. The berberine-related microbiome modulation profile is uniquely well-defined. Berberine treatment in NAFLD rodents selectively decreases the abundance of Firmicutes (Clostridiales and Lachnospiraceae) and increases the levels of Bacteroidetes and Akkermansia muciniphila [58,59]. Furthermore, enhancement of berberine increases the population of bacteria that produce short-chain fatty acids, like Bifidobacterium and Lactobacillus [58]. The above changes have been correlated with decreased levels of both fecal and systemic LPS concentrations, reestablishing intestinal tight junction protein expression, and suppression of hepatic TLR4-NF-kappaB pathway signaling [59, 60]. Importantly, efficacy of berberine in NAFLD management is dependent on the gut microbiota as its action in germ-free rodents was greatly reduced [60]. Clinical evidence in favor of berberine in the management of NAFLD/MASLD is among the most compelling for any phytochemical. In a randomized controlled trial (RCT) by Yan et al., administration of berberine 500 mg three times daily produced a significant reduction in the histological presence of steatosis, lobular inflammation, and NAS score by liver biopsy as well as normalization of serum triglycerides, LDL cholesterol, fasting glucose, and body weight (n=184, 16 weeks) [58]. Also, a systematic review and meta-analysis of 9 RCTs (n=800) revealed that berberine was highly effective against ALT, AST, total cholesterol, triglycerides, LDL cholesterol, and fasting blood glucose concentrations [60, 61].
Silymarin, standardized polyphenolic extract of milk thistle (Silybum marianum), is the most popular herb used as a hepatoprotective medicine around the world, and it is the most studied herbal compound used to treat liver diseases of all etiologies [62-66]. Silymarin is a complex containing three main flavonolignans, namely silybin (silibinin), silydianin, and silychristin, among which silybin is the most effective and predominant one (around 50–70% of silymarin's composition) [63]. There are many mechanisms by which silymarin provides protection against liver injury [63, 64]. It performs an antioxidant function via ROS scavenging, competitive inhibition of arachidonic acid peroxidation through lipoxygenase inhibition, and increase in the level of glutathione and glutathione S-transferase activity [64]. Anti-inflammatory effects include inhibition of NF-kappaB and AP-1 transcription factors, suppression of synthesis of leukotriene B4, and decrease in the content of inflammatory cytokines such as TNF-alpha, IL-6, and IL-1beta [63]. Increasing data supports the role of silymarin as a microbiota regulator. Silybin administration in high-fat diet-induced mice changes the Lactobacillus/Clostridium ratio of the gut microbiota, raises fecal SCFA levels, and strengthens the integrity of the intestinal epithelium through an increase in ZO-1 and claudin-3 expression [65, 66]. A meta-analysis performed on five RCTs (n=602) by Zhong et al. showed the effect of silymarin on ALT, AST, GGT, and total bilirubin in NAFLD patients, along with histological improvement in studies allowing liver biopsy [67]. The randomized trial by Wah Kheong et al. (n=99) showed that silymarin treatment at 140 mg TID for 48 weeks was associated with a higher rate of histological response (ALT normalization and steatosis improvement) than placebo [68].
Resveratrol is a stilbenoid polyphenol compound occurring in red grape skin, Japanese knotweed (Polygonum cuspidatum), and peanuts that mainly works via SIRT1 activation and AMPK activation [69-71]. The deacetylation of PGC-1alpha promotes mitochondrial biogenesis and energy metabolism, whereas the deacetylation of NF-kappaB p65 inhibits inflammation gene expression [70]. The activation of AMPK occurs via the LKB1 pathway and upregulation of intracellular NAD+ levels through CD38 inhibition [71]. Resveratrol controls the balance of gut microbiota composition by stimulating Lactobacillus and Akkermansia muciniphila bacteria while inhibiting Clostridiaceae and Erysipelotrichaceae, which lead to metabolic disorders [71, 72]. The influence of resveratrol on ALT, TNF-alpha, CRP, and HOMA-IR was observed to be decreased in a double-blind randomized controlled study (n=60; 12 weeks) without causing changes in liver histology at this particular dose [72]. Due to poor bioavailability, a number of delivery systems like liposomal, nanodispersed particles, and phospholipid complexes have been formulated [71]. One such bioactive compound, quercetin, is a flavonoid found in onion, caper, apple, and green tea, with potent anti-inflammatory, antioxidant, and lipid-lowering properties in MASLD models [73-75]. In terms of the mechanism involved to limit adipogenesis, quercetin modulates the Nrf2-ARE pathway, PI3K/Akt-mTOR, and PPAR-gamma signaling pathways [75]. In terms of the impact of quercetin on the gut microbiota, the consumption of quercetin helps increase intestinal permeability through the increase of Bifidobacteria levels and the decrease of Proteobacteria secreting LPS [76, 77]. The level of liver steatosis was also significantly decreased based on the image study done by Guo et al. (n=4 RCTs) [78].
Table 3. Representative clinical evidence supporting phytochemical interventions targeting MASLD-associated metabolic and inflammatory dysfunction.
|
Intervention |
Study Type |
n |
Duration |
Primary Outcome |
Key Finding |
|
Curcumin 1 g/day |
Randomized, double-blind, placebo-controlled |
102 |
8 weeks |
Liver fat (MRI-PDFF) |
Significant reduction in hepatic fat, ALT, AST; improved insulin sensitivity |
|
Berberine 500 mg TID |
Randomized controlled trial |
184 |
16 weeks |
Liver histology, lipid profile |
Reduced hepatic steatosis grade; improved TG, LDL; decreased BMI |
|
Silymarin 140 mg TID |
Double-blind placebo-controlled RCT |
72 |
6 months |
ALT normalization |
ALT normalization in 61% vs 23% placebo; fibrosis markers improved |
|
Green tea extract (EGCG) |
Pilot RCT |
45 |
12 weeks |
Liver enzymes, body weight |
ALT and AST reduction; decreased hepatic fat; anti-inflammatory effect |
|
Resveratrol 600 mg/day |
Double-blind RCT |
60 |
12 weeks |
Liver enzymes, oxidative stress |
Reduced ALT, TNF-α, CRP; improved HOMA-IR; no significant histology change |
|
Quercetin 500 mg/day |
Open-label pilot RCT |
37 |
12 weeks |
Liver fat (ultrasound) |
Significant reduction in hepatic steatosis; improved lipid profile; antioxidant effects |
Table 3: Key randomized controlled trials evaluating herbal interventions in MASLD/NAFLD with hepatic, metabolic, and inflammatory endpoints.
The strategy of “one drug-one target-one disease” which dominated pharmaceutical research and development for most of the last century is fundamentally insufficient to deal with polygenic diseases like MASLD, where the disturbance of multiple pathways plays a role [10, 12]. Network pharmacology is an interdisciplinary scientific field integrating graph theory, molecular biology, and computational chemistry to offer a formal methodology to analyze and use the polypharmacological nature of herbal compounds [12]. Networks representing diseases have been generated in network pharmacology analysis, in which each node represents a gene or protein associated with disease and each edge represents interaction between them. The mapping of herbal compound onto this network has been achieved on the basis of their targets (identified through pharmacophore modeling, molecular docking studies, and database mining), which allows for visualization of perturbation of MASLD disease network by individual compounds or by their combinations on multiple nodes [12]. It becomes evident that curcumin interacts with more than 60 MASLD-associated targets, berberine with over 40, and EGCG with around 50-polypharmacological effects unattainable by monospecific compounds [43, 56, 57].
Integration of gut microbiome compositional data (metagenomics) with host metabolomics enables construction of microbiome–metabolite–gene networks that capture the full breadth of the gut–liver axis's metabolic influence [35]. In MASLD, such integrated analyses have revealed coherent functional clusters: dysbiotic bacteria producing trimethylamine (TMA) which is hepatically oxidized to the proatherogenic TMAO by FMO3 associate with elevated cardiovascular risk independent of conventional risk factors [35]. Bile acid-producing Clostridiales species correlate with FXR suppression signatures and SREBP-1c target gene upregulation in hepatic transcriptomes, while butyrate-producing Faecalibacterium prausnitzii abundance negatively correlates with hepatic NF-kappaB activity scores [31, 38]. Metabolomics analysis of plasma and urine from MASLD patients reveals metabolite profiles indicative of disease progression, which include high concentrations of BCAAs (leucine, isoleucine, valine), products of increased microbial protein degradation, known to disrupt insulin function via activation of mTORC1 [35, 39]. High levels of aromatic amino acids (tryptophan, phenylalanine, tyrosine), synthesized by the microbiome, are observed in MASH and associated with inflammation level [79]. Herb-derived polyphenols greatly alter this network of metabolites: curcumin, berberine, and EGCG lower TMAO in plasma, correct BCAA/aromatic AA ratio, and balance the bile acid pool towards activating FXR ligands [42, 47, 56].
Incorporation of advanced omic technologies for studying the impact of herbal medicine treatments on the gut-liver axis has far-reaching consequences for both mechanistic studies and targeted therapy. Shot-gun metagenomics involves sequencing of total microbial genomes from fecal samples; this method offers an unparalleled capacity for profiling of microbiome, functional gene diversity (carbohydrate-active enzymes, bile salt hydrolases, SCFA-producing metabolic pathways), and load of antibiotic resistance genes [32, 33]. Coupling of metagenomics with metabolomics allows establishing causality between specific microbial communities, metabolite formation, and host characteristics by correlation network approach and Mendelian randomization [81]. By means of transcriptomics (RNA-seq) performed on samples of hepatic biopsies, coupled with metagenomics and metabolomics, MASLD patients treated with herbal medicines display coordinated transcription profiles: those patients with significant improvement demonstrate the normalizing effect of herbal medicine treatments on the expression of NF-kappaB targets, genes of de novo fatty acid synthesis (FASN, ACACA, SCD1), profibrotic genes (ACTA2, COL1A1, TGFB1), and increased levels of oxidative metabolism-related mitochondrial genes (PPARGC1A, CPT1A, ACADL) [82]. Moreover, scRNA-seq promises identification of Kupffer cells and hepatocyte populations with differential response to herbal medicine treatment [83].
Network analysis approaches using C-T-P (compound-target pathway) networks for herb compounds relevant to MASLD have used data from TCMSP, HERB, PharmMapper, Swiss Target Predictor, STRING, and KEGG [12]. Network analyses based on these databases reveal a conserved hub node set in the MASLD disease network representing key proteins targeted by multiple herb compounds: AKT1, TP53, IL-6, TNF, VEGFA, CASP3, MAPK1, MAPK3, RELA (p65), PPARG, and ESR1 [12, 43]. Multiple herb compounds targeting this common hub protein set provides the mechanism for the observed synergy seen when combinations of berberine and quercetin inhibit NF-kappaB activity more effectively in hepatocytes relative to individual herbs [84]. Moreover, molecular docking analyses support direct physical interactions between herb molecules and MASLD disease proteins: curcumin binds to the ATP-binding domain of IKK-beta with high affinity (-9.2 kcal/mol); berberine interacts in the DNA-binding pocket of STAT3 (-8.6 kcal/mol); EGCG interacts in the binding domain of TLR4-MD2 for LPS (-9.4 kcal/mol); and silymarin binds in the binding site for collagen in TGFBR1 (-8.1 kcal/mol) [43, 52, 57, 65]. Molecular docking data needs to be validated experimentally but can offer critical insights to optimize SAR studies.
Reestablishing a normal gut microbial balance is emerging as one of the major therapeutic goals that lie mechanistically upstream of subsequent hepatic damage in MASLD [26]. Herbal components act on the microflora via several direct and indirect pathways. The direct antimicrobial effects of curcumin, which disrupt the membranes of Gram-negative bacteria producing LPS, the disruption of bacterial FtsZ polymerization by berberine (a process vital for bacterial division), and the inhibition of bacterial dihydrofolate reductase by EGCG target pathobiont microflora selectively without causing the collateral dysbiosis observed with broad-spectrum antibiotics [42-47, 56].
Indirect modifications to the microbiota occur via host-mediated actions; upregulated intestinal production of defensins, IgA, and mucins promote a favorable intestinal milieu for commensal flora [26, 47]. Herbal prebiotics, such as inulin-type fructans and arabinoxylans found in most medicinal plants, directly enhance Bifidobacterium and Lactobacillus growth and increase SCFA secretion and competition against pathobionts [82]. This microbial balance is self-perpetuating because increased levels of Akkermansia strengthen the mucus layer, making it less permeable to pathobionts and preventing LPS translocation [26, 80, 81].
A critical mechanism by which herbs help in the treatment of MASLD is the restoration of integrity in tight junctions within the intestinal epithelium. Curcumin is found to increase expression of ZO-1, claudin-1, and occludin in cultured intestinal epithelial cells and in vivo NAFLD models via suppression of NF-kappaB (resulting in removal of transcriptional inhibition of ZO-1) and activation of cAMP-PKA signaling pathways [47, 48]. Berberine has especially notable effects on intestinal barrier functioning, promoting ZO-1 and E-cadherin expression while decreasing paracellular permeability based on FITC-dextran transport experiments via AMPK-dependent pathways which increase MLCK regulation [85].
EGCG increases tight junction integrity by means of EGF receptor-PI3K signaling pathway and modulating the activity of Rho GTPases, resulting in stabilization of the actin cytoskeleton upon which tight junction proteins attach [52]. The benefits of silymarin against liver injury include increased tight junction integrity by means of Nrf2 activation which results in elevation of glutathione and heat shock protein levels in enterocytes, thus decreasing damage from oxidative stress [65, 66]. Overall, the consequence of herbal intervention in regard to intestinal permeability is a decrease in portal LPS levels which prevents activation of TLR4-NF-kappaB pathway.
Multi-targeted inflammatory pathway suppression is one of the major hallmarks of the pharmacological mechanism of herbal compounds in MASLD [45, 46, 63]. Inhibition of NF-kappaB transcription factors through the following approaches: inhibition of IKK-beta kinase activity (curcumin), p65 transcription factor acetylation (resveratrol through SIRT1), inhibition of AMPK-mediated IKK-beta phosphorylation (berberine), and TAK1 kinase inhibition (EGCG) suppresses the transcription of TNF-alpha, IL-6, IL-1beta, iNOS, and COX-2 transcription. Inflammasome inhibition by curcumin, EGCG, and resveratrol suppresses IL-1beta and IL-18 maturation and hepatocyte pyroptosis [86]. Anti-inflammatory cytokine secretion is also stimulated by the use of herbal compounds, as demonstrated by the increase of hepatic and intestinal IL-10 cytokines in response to curcumin and resveratrol consumption [71]. Expansion of regulatory T-cells due to an increased production of SCFAs caused by microbiota normalization is another way of reducing hepatic and intestinal inflammation [38, 39].
Normalization of liver lipid metabolism dysfunction is another key therapeutic goal that herbal compounds can achieve via complementary strategies involving lipid biosynthesis and oxidative metabolism [57, 58, 71]. AMPK activation by berberine, EGCG, and resveratrol inhibits SREBP-1c expression while increasing PPAR-alpha-mediated expression of carnitine palmitoyltransferase-1 (CPT1A) and medium-chain acyl-CoA dehydrogenase (MCAD) enzymes, facilitating fatty acid transportation into mitochondria for their oxidative breakdown.
Curcumin and silymarin inhibit liver cholesterol synthesis via HMG-CoA reductase inhibition and increasing LDL receptors on hepatocyte membranes, thus decreasing liver cholesterol content [65]. Clinical relevance of the mentioned above effects of herbs on liver lipid metabolism is demonstrated in the reduction of serum triglycerides, LDL, and non-HDL in RCTs with berberine, curcumin, EGCG, and silymarin, and decreased liver fat content confirmed by ultrasonography and MRI [72].
Modulation of bile acid signaling via herbs is an underappreciated yet highly significant therapeutic mechanism for MASLD [40, 41]. In addition to direct receptor stimulation, berberine modulates the bile acid pool composition towards stronger FXR and TGR5 agonists (e.g., CDCA and UDCA) through inhibition of bacterial bile salt hydrolases and increased efficiency of primary bile acid conjugation [60]. FXR activation downregulates the CYP7A1 pathway responsible for the synthesis of bile acids, which ensures a more normal concentration of hepatotoxic substances and prevents triggering of NLRP3 inflammasomes [87]. The TGR5-dependent effect of secondary bile acid pool optimization induced by the herbal treatment leads to increased release of GLP-1 by L-cells in the intestines, leading to a better postprandial response of the insulin-producing system and lowering glucose production in the liver. In addition, activation of type 2 deiodinase in brown adipose tissue through stimulation of the TGR5 pathway increases the concentration of triiodothyronine (T3), thereby promoting energy expenditure and thermogenesis, which complements the lipid-lowering activity of the herb-derived compounds in the liver [88].
Table 4. Major signaling pathways and molecular targets influenced by phytochemical interventions in MASLD.
|
Target |
Biological Function |
Role in MASLD |
Herbal Modulators |
Therapeutic Effect |
|
FXR (NR1H4) |
Nuclear bile acid receptor regulating bile acid homeostasis |
Suppressed FXR leads to increased lipogenesis and inflammation |
Berberine, EGCG, Silymarin, Ginsenoside |
Restore bile acid homeostasis; reduce hepatic fat; suppress inflammation |
|
TGR5 (GPBAR1) |
G protein-coupled bile acid receptor; stimulates GLP-1 secretion |
Reduced TGR5 activity impairs glucose metabolism and energy expenditure |
Berberine, Curcumin, Ursodeoxycholic acid |
Enhance energy expenditure; improve insulin sensitivity |
|
TLR4 |
Pattern recognition receptor for LPS on Kupffer cells |
Excessive LPS activation drives NF-κB-mediated hepatic inflammation |
Curcumin, Berberine, Baicalin, EGCG |
Block LPS-TLR4 interaction; suppress NF-κB activation |
|
NF-κB |
Transcription factor regulating pro-inflammatory genes |
Chronically activated in MASLD driving TNF-α, IL-6, IL-1β production |
Curcumin, Quercetin, Resveratrol, Silymarin |
Reduce cytokine production; attenuate hepatic inflammation |
|
AMPK |
Master energy sensor regulating lipid and glucose metabolism |
Suppressed in MASLD; leads to increased lipogenesis, reduced β-oxidation |
Berberine, Resveratrol, EGCG, Quercetin |
Activate fatty acid oxidation; suppress SREBP-1c; improve insulin signaling |
|
Nrf2 |
Transcription factor for antioxidant response elements |
Impaired Nrf2 activation contributes to oxidative stress and mitochondrial dysfunction |
Curcumin, Silymarin, Resveratrol, Quercetin |
Upregulate HO-1, NQO1; reduce ROS; protect hepatocytes |
|
PPAR-α |
Nuclear receptor regulating fatty acid oxidation |
Decreased PPAR-α activity promotes hepatic lipid accumulation |
EGCG, Berberine, Curcumin |
Enhance mitochondrial fatty acid β-oxidation; reduce hepatic steatosis |
|
SIRT1 |
NAD+-dependent deacetylase; regulates metabolism and inflammation |
Reduced SIRT1 activity promotes lipogenesis and inflammatory gene expression |
Resveratrol, Quercetin, Curcumin |
Deacetylate NF-κB, FOXO1; improve lipid metabolism |
Table 4: Principal molecular targets engaged by herbal bioactive compounds in MASLD, with associated biological functions, disease roles, and therapeutic outcomes.
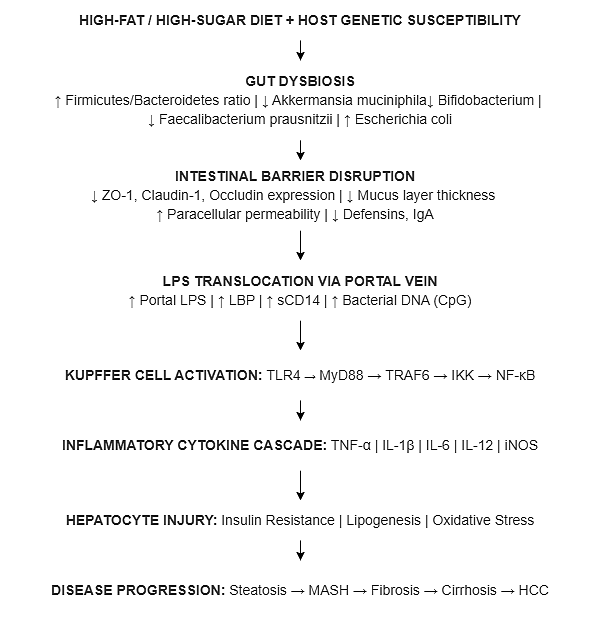
Figure 1: Gut Dysbiosis to Hepatic Injury Cascade in MASLD
Figure 1: Stepwise pathogenic cascade linking gut dysbiosis to progressive hepatic injury in MASLD, highlighting molecular intermediaries and intervention points for herbal therapeutics

Figure 2: Herbal Intervention Points in the MASLD Gut-Liver Axis
Figure 2: Schematic representation of the multi-level intervention profile of major herbal compounds across the gut microbiome, intestinal barrier, and hepatic signaling axes in MASLD
DISCUSSION
The convergence of systems biology, studies on gut microbiota, and phytopharmacology has provided us with an inspiring scientific paradigm, wherein the potential of using herbal remedies as therapies for MASLD has been highlighted. The multipathogeneses involved in MASLD, which include gut dysbiosis, intestinal barrier dysfunction, endotoxemia-induced inflammation, deregulation of bile acid signaling, insulin resistance, oxidative stress, and fibrogenesis, favor multi-target therapies over single-target drug therapy [7,10,12]. Herbal compounds through their evolutionary selection as multi-ligand effectors in competitive ecological environments possess precisely the polypharmacological profiles required to engage this complex pathogenic network at multiple nodes simultaneously. The clinical evidence base for herbal interventions in MASLD, while promising, retains important limitations. The majority of positive RCT findings derive from trials of limited sample size and duration, frequently using surrogate biochemical endpoints (liver enzymes, lipid profiles) rather than the histological benchmarks reduction in NAS score, fibrosis stage, or resolution of MASH - that regulatory agencies require for approval [42, 58, 66, 72]. Variability in study design in terms of composition and standardization of herbal extracts, administration dosing regimen, population groups involved, and concomitant therapies creates obstacles in the interpretation and meta-analysis [63, 65]. Oral bioavailability remains a major pharmacokinetic barrier, as oral absorption of curcumin in standardized formulations is less than 1% and that of EGCG is greatly diminished by food interactions; therefore, formulation optimization will be required to achieve clinical utility [43, 51]. Gut microbiota is shown to act both as a mediator of pathology and a main target of herbal compounds' action in MASLD pathogenesis, as the latter have demonstrated consistent normalizing effect on the gut microbiota composition, which correlates with their hepatoprotective properties [87]. The dependence of berberine-induced metabolic benefits on an intact microbiome in germ-free mice models emphasizes the significance of studying herb-drug interactions at the microbiome level [60]. More studies are required for the better understanding of the molecular mechanisms involved in the positive effects of herbs through systems biology-based approach by using metagenomics, metabolomics, and transcriptomics. It must be noted that herbal medications also have their own risks regarding pharmacovigilance. The interaction of herbal medicine with other drugs remains a vital concern for individuals who are under the influence of other prescribed drugs for other ailments [62]. The ability of berberine to inhibit cytochrome P450 3A4 and P-glycoprotein affects the metabolism of other drugs such as cyclosporin, statins, and warfarin. Silymarin, despite its overall good tolerability profile, has some reports in standardized reporting systems that show the risk of hepatotoxicity. The platelet aggregation inhibitors present in curcumin complement the effects of anticoagulants [88].
CONCLUSION
MASLD is a multifaceted metabolic-inflammation disease where the gut-liver axis plays a central role in mediating the crosstalk between microbial ecology, gut barrier integrity, bile acid signaling, and activation of innate immune system within the liver. Herbal medicines like curcumin, berberine, EGCG, silymarin, resveratrol, and quercetin have an impressive array of biological properties that are perfectly aligned with the mechanism of MASLD pathogenesis involving microbial ecology, gut barrier integrity, TLR4-NF-kappaB signaling, FXR/TGR5 bile acid receptors, AMPK/Nrf2/SIRT1 metabolic pathways, and fibrogenesis. Systems Biology and Network Pharmacology approaches to studying MASLD have firmly justified the scientific rationale behind herbal medicine in treating MASLD and provided a framework for finding the best combination of drugs and predicting individual response to treatment. Metagenomic, metabolomic, and transcriptomic approaches will make an enormous contribution into the future of herbal medicine by providing evidence for efficacy and helping us find biomarkers of responsiveness and causality in normalization of the gut-microbiome-gut-liver axis.
Specific recommendations to move the field forward should be to conduct:
If this research agenda is achieved, herbal medicine would be established as a scientific and mechanistically guided complement to mainstream treatment of MASLD.
REFERENCES

Ashutosh Rana*, Gut - Liver Axis and Herbal Therapeutics in MASLD: A Systems Biology Perspective, Int. J. Med. Pharm. Sci., 2026, 2 (6), 472-492. https://doi.org/10.5281/zenodo.21057234
 10.5281/zenodo.21057234
10.5281/zenodo.21057234