
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1P. G. Scholar, Department of Homoeopathic Materia Medica, Mahesh Bhattacharyya Homoeopathic Medical College and Hospital, Government of West Bengal, India
2Junior Research Fellow, Peripheral Pharmacovigilance Centre, Mahesh Bhattacharyya Homoeopathic Medical College and Hospital, Government of West Bengal, India
3Ex Reader. Department of Organon of Medicine, Metropolitan Homoeopathic Medical College & Hospital, West Bengal, India
4P. G. Scholar, Department of Case Taking and Repertory, Mahesh Bhattacharyya Homoeopathic Medical College and Hospital, Government of West Bengal, India
5Assistant professor, Department of Homoeopathic Materia Medica, Burdwan Homoeopathic Medical College and Hospital, West Bengal, India
6Junior Research Fellow(H). Clinical Research Unit(T), For Homoeopathy, Gangtok Sikkim, Under CCRH, Ministry of AYUSH, Govt. of India
Vitiligo is an idiopathic depigmentation disorder of skin that results in marked reduction or even absence of melanocytes and melanin in the epidermis. Autoimmune, biochemical and oxidative stress, genetic, neuronal and environmental factors are thought to interact and contribute to the development of vitiligo. It can severely impact in patient’s quality of life both physically and psychologically. Case summary: A 30-year-old male patient suffering from vitiligo for six months presented with depigmented patches on both sides of the eyes and neck region. After a thorough clinical evaluation, Staphysagria in increasing potency (up to MK), was prescribed during the follow-up visits and lastly the treatment was ended by prescribing the anti-psoric medicine Sulphur. The impact of the disease and its treatment on quality of life and the outcome were assessed using Vitiligo impact scale – 22 (VIS-22). Marked improvement was found in the depigmented lesions evidenced photographically and the VIS-22 scores showed significant reduction affirming the same. The MONARCH score (+9) suggested that the clinical improvement was likely attributable to the homoeopathic treatment. This evidence-based case report suggests a beneficial role of homoeopathy in the treatment of vitiligo.
Vitiligo is an acquired idiopathic depigmenting disorder of the skin and mucosa, affecting around 0.5% to1% of the population worldwide1. Although vitiligo is found all across the world, it is most prevalent in India, Egypt and other tropical countries2.The incidence is highest among Indians from the Indian subcontinent, followed by Mexico and Japan3. The disorder affects both adults and children of both sexes, but females are more likely to suffer from it, most likely due to a lot of social stigmas 4. Vitiligo is mostly associated with psychological distress. Numerous studies demonstrate that vitiligo patients experience a lot of social stigmas, low self-esteem, adjustment disorder, poor body image, and a poor quality of life 4-6. Even though vitiligo is typically thought of as a cosmetic issue, it can coexist with a number of other autoimmune disorders such as Hashimoto thyroiditis, Celiac disease, Scleroderma, Rheumatoid arthritis, Psoriasis, Addison’s disease, Pernicious anaemia, SLE, Diabetes type – I, Alopecia areata etc 7-9. Vitiligo is classified into two major types, segmental and non-segmental, with the latter including several subtypes (generalized vitiligo, acrofacial vitiligo, and universal vitiligo). Segmental vitiligo (SV) is characterized by its early onset, rapid stabilization, and unilateral distribution 1, whereas non-segmental vitiligo is often distributed symmetrically on the body and progresses slowly over time 10. Although the precise aetiology of vitiligo is unknown, current research suggests that it is caused by a complex interplay between autoimmunity, oxidative stress, and genetics 11. Various systems of medicine have claimed to have good results in cases of vitiligo. There are many cases documented in homoeopathic journals regarding the therapeutic efficacy of homoeopathic medicines in the treatment of vitiligo 12-18. This case report demonstrates, positive role of homoeopathic medicine, Staphysagria, in treatment of a case of vitiligo. After the medication gradual and progressive re-pigmentation was visible and there is no recurrence of symptoms within seven to eight months of follow-up. Individual curative response of a homeopathic medicine was assessed in the case using Modified Naranjo Criteria for Homoeopathy-Causal Attribution Inventory 19, which further elucidated the role of individualised treatment in homoeopathy. Assessment of cases were done using Vitiligo impact scale – 22 (VIS-22) 20.
CASE REPORT
Patient information
A 30-year-old male patient exhibited multiple hypopigmented patches across his body for the past six months, with larger patches around both eyes (predominantly on the left side) and the neck region (Figure 1 a-c). He had no significant medical history since childhood and had not sought any prior medical treatment for these complaints.
Clinical findings
During the examination, depigmented patches were observed around the left eye and neck region. The patient initially experienced itching, followed by redness. Over time, white depigmented patches appeared in those areas. The patient reported a history of recurrent styes on both the eyes during his childhood. The patient revealed inadequate appetite, a preference for cold foods, eggs, and pungent flavours, though he suffered from sour eructations along with foul breath. The patient exhibited diminished thirst. Irregular, malodorous, hard bowel movements with ineffectual urging and straining occurred at an interval of 2 - 3 days, with an urging for frequent urination while the patient slept soundly. Moreover, the patient expressed intolerance to extreme temperatures, with scanty perspiration across the entire body. While narrating his complaints, the patient exhibited anxiety. He also disclosed a history of suppressed emotions from approximately six months ago, during which his family members frequently noted his anger and irritability over minor matters.
Diagnostic assessment
The patient exhibited depigmented patches on the face, primarily around the left eye and extending throughout the neck region. There was no reported family history of similar depigmented spots. Thyroid Function Test results (T3, T4, TSH) were within the normal range. Based on the patient’s history and clinical examination, a diagnosis of vitiligo was established [ICD 11 classification code ED63. 0].
Therapeutic intervention
Totality of symptoms
The totality of symptoms for the above-mentioned case is listed below:
Case analysis and repertorisation
After a detailed case-taking, totality was constructed considering past history, characteristic physical general and particular symptoms. The miasmatic evaluation of all the presenting symptoms of this case mostly indicated psoric manifestations 21, as shown in Table 1.
Table 1: Miasmatic analysis
|
Sl. No. |
Symptoms |
Miasm corresponding |
|
1. |
Depigmented patches over the face and neck |
Pseudo psora |
|
2. |
History of suppressed emotion |
Psora |
|
3. |
Anxious; Irritable |
Psora |
|
4. |
History of recurrent styes during childhood |
Sycosis |
|
5. |
Complaint of sour eructations |
Psora |
|
6. |
Thirstless |
Psora |
|
7. |
Irregular, malodorous, hard bowel movements with ineffectual urging and straining |
Psora |
|
8. |
Urging for frequent urination |
Psora |
In this case, after analysing the characteristic mental and physical symptoms taken from the totality of symptoms repertorisation was carried out by Hompath Zomeo pro version using Kent’s repertory. After repertorisation, the top ranked medicines came out to be Staphysagria (19/7), Sepia officinalis (15/8), Sulphur (15/6), Pulsatilla (15/5), Lycopodium clavatum (14/6). Repertorial result are shown in (Figure 2). After considering the reportorial result, miasm, and homoeopathic Materia Medica 22,23 Staphysagria was selected and other remedies were ruled out. The selection of potency and dosage was done following the guidelines of the Organon of Medicine 24. The first prescription, Staphysagria 200C, two doses were prescribed on 13 April 2015. The patient was advised not to apply any ointment.
Follow-up and outcome
The patient was followed-up and assessed for nearly about four years. The medicine, i.e. Staphysagria was continued up to MK potency, and there was a marked diminution of the depigmented patches across the body of the patient. Although the depigmented patches were reduced to a great extent, but still the patient was not fully recovered and after few months, patient reported appearance of a new hypopigmented spot on the left side of the face. Re-case taking was done, and according to the indications and available totality of the symptoms, Sulphur 200C/ 2 doses were prescribed. Since then, placebo was prescribed in response to the patient’s progressive improvement. All hypopigmented patches over the face and neck were cleared except for the spot on the right leg, which although decreased in size. No adverse events or homoeopathic aggravation noted at the end or while the patient was under treatment. The details of the follow-ups are given in Table 2.
Table 2: Follow-ups of the case
|
Date of visit |
Observations |
Prescription |
VIS-22 score |
|
13/04/2015 |
Multiple depigmented patches around both eyes (predominantly on the left side) and the neck region for the past six months (Figure 1a-c). |
Staphysagria 200C/2D |
41 |
|
10/06/2015 |
The depigmented patches remained largely unchanged, with no signs of repigmentation. The patch margins remained stable, and there was no associated itching or redness in the affected area. |
Placebo200C/30D |
41 |
|
09/07/2015 |
Some pigment spots were observed on the patches, indicating improvement in the patient’s condition (Figure 3 a-b). |
Placebo 200C/30D |
38 |
|
10/08/2015 |
The patches in the affected areas showed significant improvement (Figure 4 a-b). |
Placebo 200C/30D |
30 |
|
08/09/2015 |
The patient showed improvement, and depigmented patches were also decreasing, as evident from the photographs. (Figure 5 a-c) |
Placebo 200C/30D |
26 |
|
05/09/2016 |
Afterward, the patient did not return for a year but then reported on September 5, 2016. Notably, the white spots around the left eye had cleared but persisted on the neck region (Figure 6 a-b). Upon reviewing the totality of symptoms, they remained largely unchanged. |
Placebo 200C/30D |
26 |
|
03/10/2016 |
The white spots on the anterior part of the neck persisted, with no new spots on the body. |
Staphysagria MK/2D |
22 |
|
03/08/2017 |
The depigmented patches on the front of the neck remained unchanged, without any appearance of new spots elsewhere on the body. |
Staphysagria MK/2D |
20 |
|
17/11/2017 |
The white spots showed improvement, and the patches on the right side of neck as well as around the left eye, cleared (Figure 7 a-b). |
Placebo 200C/30D |
18 |
|
20/03/2018 |
The depigmented patches on the front of the neck diminished to a great extent (Figure 8). |
Staphysagria MK/2D |
18 |
|
06/05/2018 |
The patches remained stable, but the patient noticed a new white spot on the left side of the face the previous day (Figure 9 a-b). Upon reviewing the symptoms, we observed hot palms, increased thirst, and a craving for sweets. Considering the failure of the previously indicated remedy, we prescribed Sulphur 200. |
Sulphur 200C/2D |
18 |
|
19/01/2019 |
All white spots on the face and neck almost cleared (Figure 10 a-d). |
Placebo 200C/30D |
16 |
|
The physician also advised the patient to visit the clinic every 3 months to check for recurrence of vitiligo, the patient came for follow-up for 7-8 months, did not report of any recurrence of old complaints and the generals were also normal. |
|||
Further, utilising the Vitiligo impact scale – 22 (VIS-22) 20, the patient-reported outcome was quantified. The VIS-22 scores steadily improved and were confirmed as much better after using the prescribed homoeopathic medications. The 22 items in VIS-22 are divided into several domains viz., attitude (questions 1, 4, 17, 19), anxiety (2, 11), social interactions (3, 12, 13), self-confidence (5, 18), depression (6, 9, 10, 14), treatment (7, 15, 16), family (8), marriage (20), employment (21) and education (22). On a scale of 0 to 3, each question is worth 0 for not at all, 1 for a little, 2 for a lot, and 3 for very much. Higher total scores suggest a greater impact on life, and the score ranges from 0 to 66 20. In this case, VIS-22 score was reduced from 41 to 16. The Modified Naranjo Criteria are applied to this case for ascertaining the causal attribution between the homoeopathic medicine applied and the changes in the symptoms/signs of the patient Table 3 19. The total score of the outcome is (+9).
Table 3: Assessment done by MONARCH Inventory score
|
Domains |
Yes |
No |
Not Sure /NA |
|
1. Was there an improvement in the main symptom or condition, for which the homoeopathic medicine was prescribed? |
+2 |
- |
- |
|
2. Did the clinical improvement occur within a plausible time frame relative to the drug intake? |
+1 |
- |
- |
|
3. Was there a homoeopathic aggravation of symptoms? (need to define in glossary) |
- |
- |
0 |
|
4. Did the effect encompass more than the main symptom or condition, i.e., were other symptoms, not related to the main presenting complaint, improved or changed)? |
+1 |
- |
- |
|
5. Did overall well-being improve? (suggest using a validated scale or mention about changes in physical, emotional and behavioural elements) |
+1 |
- |
- |
|
6: (A) Direction of cure: Did some symptoms improve in the opposite order of the development of symptoms of the disease? |
- |
0 |
- |
|
6: (B) Direction of cure: Did at least one of the following aspects apply to the order of improvement of symptoms: From organs of more importance to those of less importance? From deeper to more superficial aspects of the individual? From the top downward? |
- |
0 |
- |
|
7. Did “old symptoms” (defined as non-seasonal and non-cyclical symptoms that were previously thought to have resolved) reappear temporarily during the course of improvement? |
- |
0 |
- |
|
8. Are there alternate causes (other than the medicine) that – with a high probability – could have caused the improvement? (consider known course of disease, other forms of treatment and other clinically relevant interventions) |
- |
+1 |
- |
|
9. Was the health improvement confirmed by any objective evidence? (e.g., investigations, clinical examination, etc.) |
+2 |
- |
- |
|
10. Did repeat dosing, if conducted, create similar clinical improvement? |
+1 |
- |
- |
|
Total score = + 9 (Maximum score = +13, minimum score = - 6) |
|||
DISCUSSION
The case report describes the utility of homoeopathic treatment in the management of vitiligo. This case of vitiligo presented with multiple hypopigmented patches on different parts of the body has improved with individualised homoeopathic treatment. This case serves as an example of external one-sided disease (Local disease) which are not the manifestations of the local part but of the whole individual as mentioned in the Organon of medicine 24. Dr. Hahnemann has mentioned that, to treat the one-sided disease one has to consider he person who is sick, not the part of the body and therefore it is the sick person who is to be treated not a single part. In this case an attempt has been made to evaluate the complaints of the patient from the perspective of the whole person—physically, mentally, and emotionally. Then, an individualised homoeopathic remedy was selected from the totality of symptoms to not only promote ‘gentle healing but also provide a speedy recovery 24. In the above case of Vitiligo, the remedy Staphysagria was selected based on analysis of the constitutional totality, repertorisation (Figure 2) and consultation with Materia Medica. Initially, the remedy Staphysagria was given in 200th potency and patient showed progressive improvement. Thereafter patient discontinued the treatment and turned back after 1 year. At that time, the white spots around the left eye had cleared but persisted on the neck region although he did not use any other medication during this period (Figure 6 a-b). Later, during the subsequent visit the same medicine was given in the next higher potency, MK, as there was no further improvement and Staphysagria still seemed to be indicated based on the available totality. Post medication, gradual improvement in the main complaint, as well as overall well-being was observed over a considerable period of time. Staphysagria MK was repeated twice at the next two-year follow-up visits. However, at a subsequent visit, patient reported appearance of a new white spot on the left side of the face although the other patches remained stable. At this point, the case was reassessed and considering the lack of improvement even after the well-selected remedy, the recurrence of the complaints and the presenting totality two doses of Sulphur in 200th potency was prescribed. Considering the symptomatology and pathology, the case appeared to have a Psoric predominance 25. Sulphur is considered as the king of anti-psoric remedies and after consulting with Materia Medica 22 it was found that Sulphur has a follows-well relationship with Staphysagria, which means it does not harm or act unfavourably against the previous remedy. These two points were also considered during the selection of the medicine. The patient improved markedly with this remedy. The depigmented spots on his face and neck were almost completely disappeared (Figure 10 a-d). The criteria for assessing the response to the treatment of vitiligo include cessation of spread; the appearance of skin re pigmentation; and an overall improvement of quality of life during treatment 26. In this case, all these criterias were met and the improvements were documented through different subjective and objective pieces of evidence. Improvement in the local lesions is evident from the substantial reduction in the VIS-22 score 20 from the baseline value of 41–16 by the end of the follow-up. As per the modified Naranjo Criteria 19, there was an improvement in the primary symptom (+2); within a plausible timeframe after the intake of medicine (+1); with an improvement in other symptoms (+1) and overall well-being (+1); with no other alternative causes that could have caused the improvement (+1). Further, there was an objective improvement in the skin lesions after the remedy, evidenced by photographs and VIS-22 score (+2). The remedy, on repetition of dose, has resulted in a similar clinical improvement (+1). Thus, in this case, the total score of +9 out of the highest score of +13 establishes a definite causal attribution of homoeopathic treatment with the outcome. Thus, the case reemphasises the usefulness of individualised homoeopathic treatment in the management of vitiligo.
CONCLUSION
This case demonstrates a positive outcome with homoeopathic treatment of vitiligo without any recurrence. Further, rigorous well-designed studies are warranted with an adequate sample size to corroborate the findings.
REFERENCES

Figure 1 – (As on 13 April 2015): (a) left side of eye (b) left side of neck (c) right side and front of neck
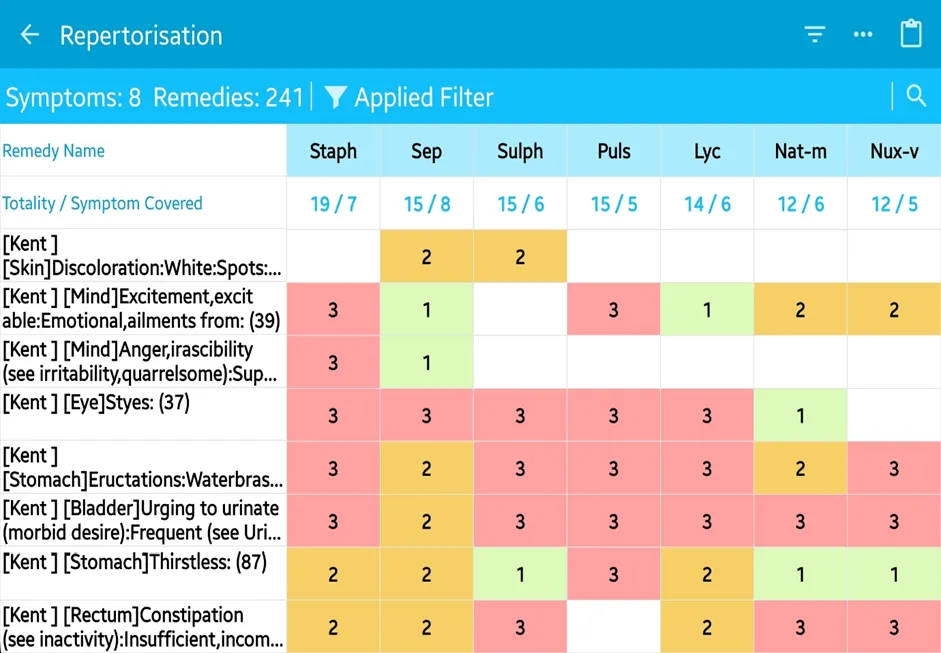
Figure 2 – Repertorisation sheet

Figure 3 – (As on 9 July 2015): (a) left side of eye (b) left side of neck

Figure 4 – (As on 10 August 2015): (a) left side of eye (b) left side of neck

Figure 5 – (As on 8 September 2015): (a) left side of eye and left side of neck (b) right side of neck (c) front of neck

Figure 6 – (As on 5 September 2016): (a) left side of eye (b) front of neck

Figure 7 – (As on 17 November 2017): (a) left side of eye (b) right side of neck

Figure 8 – (As on 20 March 2018): front of neck

Figure 9 – (As on 6 May 2018): (a) left side of eye (b) front of neck

Figure 10 – (As on 19 January 2019): (a) left side of eye (b) left side of neck (c) right side of neck (d) front of neck







Abhisek Hui, Shankhadeep Pal, Subimal Krishna Saha, Debojyoti Singha, Santana Maity, Aditi Biswas, Shankha Subhra Patra*, Staphysagria’s Therapeutic Potential in the Treatment of Vitiligo: A Case Report, Int. J. Med. Pharm. Sci., 2026, 2 (7), 369-377. https://doi.org/10.5281/zenodo.21257620
 10.5281/zenodo.21257620
10.5281/zenodo.21257620