
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Vidyaniketan College of Pharmacy, Anjangaon Surji, Amravati, Maharashtra 44470
Lacerations are among the most common traumatic injuries and are associated with pain, inflammation, risk of infection, and delayed wound healing. Effective management requires prompt wound assessment, haemostasis, infection control, and appropriate closure techniques to promote tissue repair and minimize complications. Conventional therapies, including antiseptics, antibiotics, analgesics, non-steroidal anti-inflammatory drugs (NSAIDs), and suturing methods, remain the cornerstone of treatment but may be associated with adverse effects and increased treatment costs. Herbal therapies have gained considerable attention as complementary alternatives because of their anti-inflammatory, antimicrobial, antioxidant, and wound-healing properties. Medicinal plants such as Aloe vera, Curcuma longa (turmeric), Azadirachta indica (neem), Ocimum sanctum (tulsi), and Moringa oleifera contain bioactive compounds that enhance collagen synthesis, stimulajte fibroblast proliferation, reduce oxidative stress, and accelerate tissue regeneration. This review summarizes the pathophysiology of laceration healing, conventional treatment approaches, and the therapeutic potential of herbal medicines in improving wound healing outcomes.
Introduction of Laceration:
One of the most frequent conditions is laceration issues in the emergency room. In 1996, nearly IN emergency departments, 11 million wounds were treated during Americas. One On average, each patient costs $200.This amounts to over $2 billion every year. The fundamentals of wound care haven't changed all that much throughout the years. While the majority of cuts heal withoutsequelae regardless of management, mismanagement may cause uncomfortable and dysfunctional scars, wound infections, extended convalescence, and, very Mortality [1] Lacerations are one of the most common types of traumatic injuries, characterized by the tearing of the skin and underlying soft tissues. These injuries can result from accidents, falls, sharp objects, or blunt trauma the severity of lacerations can range from minor superficial cuts to deep wounds involving muscles, tendons, nerves, and blood vessels. Such injuries not only compromise the structural integrity of the skin but also increase the risk of infection, delayed healing, and functional impairment [2] The body’s response to a laceration is marked by inflammation, a complex physiological and cellular process aimed at eliminating damaged tissue, preventing infection, and initiating repair At the cellular level, the inflammatory response involves the recruitment of neutrophils, macrophages, and other immune cells to the injury site. These cells release cytokines, chemokines, and growth factors that regulate the healing process. Additionally, reactive oxygen species (ROS) and proteolytic enzymes help clear pathogens and necrotic tissue, preparing the wound bed for regeneration Laceration healing progresses through three overlapping phases:1.Inflammatory phase: Immediately after injury, haemostasis occurs, followed by infiltration of immune cells to remove debris and prevent infection Proliferative phase: Fibroblasts proliferate, collagen is deposited, angiogenesis occurs, and epithelial cells migrate to cover the wound. Remodelling phase: Collagen fibres reorganize, tissue gains tensile strength, and functional integrity is gradually restored [3,4]
Factors: of laceration
Growth Factor:
Acute inflammation is necessary for healing, but prolonged or excessive inflammation can impede repair.
Age:
The number of elderly people (those over 60) is increasing. more quickly other age group, according to the WHO [World Health Organization, www.who.int/topics/aging]), and growing older is significant risk factor for poor wound healing [5,6]
Inflammation:
The body's immune system's biological reaction to damaging stimuli like infection, tissue damage, or poisonous substances is inflammation. This procedure's main goals are to eliminate dangerous substances, remove damaged tissue, and start the healing process [7] Inflammatory stimuli like cytokines and bacterial endotoxins cause COX-2 to be released. The molecular target of medications that reduce pain and inflammation. The conversion of phospholipids to arachidonic acid In reaction to tissue damage and are subsequently converted by COX into PGE2. Enzymes. PGG2 is created when cyclooxygenase gives arachidonic acid two oxygen molecules. By peroxidation, which is subsequently committed to PGH2. Eventually, PGE2s and PGE synthase is activated to produce additional prostaglandins [8] The condition of inflammation is a Pathophysiological expression of many illnesses. The innatate immune system is triggered as soon as an injury occurs initiating a regional inflammatory reaction that involves the enlistment of circulatory cells that cause inflammation. The degranulation is the first step in this quick reaction. of platelets that reach the location and the resident mast's degranulation brought on by injury cells. Resident macrophages and other local immune cells are triggered by mediators of inflammation released in reaction to damage additionally encourages inflammation because hypoxia activates a variety of cell types, including macrophages, to generate inflammatory mediators. In reaction to these numerous signals, leukocyte chemoattractant levels significantly rise, and further boosting the recruitment of leukocytes [9]
Laceration Closer Techniques:
|
Techniques |
Comments |
|
Simple sutures that have been interrupted |
Approximation of general tissue Suitable for the majority of woundsnBasic running sutures [10,11] |
|
Basic running sutures |
Quick and efficient for lengthy cuts [10,11] |
|
Sutures for a vertical mattress |
Best for everting the edges of wounds may result in skin necrosis. [10,11] |
|
Mattress sutures partially buried |
Most useful for correcting flap errors in triangular wound edges [10,12] |
|
Subcuticular suture running |
Accurate skin edge positioning that is quick and efficient does not permit drainage Suitable for suturing clean wounds, like surgical wounds in medical rooms. [10,11] |
|
Defective sutures were interrupted.
|
Efficient in wound eversion and precise skin edge apposition permits minimal drainage conditions for the closure of clean wounds. [10,11] |
|
Staples adhesive
|
Quick, results in a loose closure permits drainage Suitable for dirty wounds Avoid if you want cosmetic results. Is Vital. [10,11] |
|
Adhesive strips for wounds
|
Quick and anaesthesia-free used with minimal strain and without bleeding to approximate simple, clean, minor cuts. [10,11] |
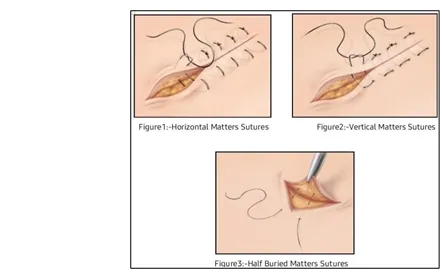
Figure 1: Sutures
Evaluation of Wound:
This medication is commonly prescribed for pain resulting from inflammation Our body has a system of natural chemicals that regulates pain. The dorsal horn, brain stem, and peripheral tissue fibres release natural opioids and neurotransmitters that stop the manner in which neurons transmit pain impulses. play a significant role in primary healthcare. Natural substances called endorphins are similar to opioids and are to ease discomfort. When a patient arrives with a cut, the doctor should examine the wound's size, shape, and location after getting a history that includes the patient's allergies, tetanus vaccination status, and the mechanism of injury. Prior to further assessment, haemostasis should be achieved using haemostatic if active bleeding continues after direct pressure has been applied. Haemostasis controls bleeding, stops hematoma formation, and permits a more thorough examination of the wound. Finding out if there is damage to the joints, muscles, tendons, nerves, vessels, or bones comes next. In order to explore the wound and achieve haemostasis, anaesthesia might be required. To lower the risk of inflammation, devitalized and necrotic tissue in a traumatic wound should be located and removed. Suture-requiring lacerations are a contributing factor in as many as half of children with injuries who visit the emergency room. Despite tissue adhesives being readily available, many still Need to be sutured. [12,13]
METHODS AND MATERIAL:
Conventional Therapy:
Patients with Crohn’s disease may benefit from better treatment outcomes and a change in the disease’s progression with biologic and other innovative therapies that target particular pathogenic processes [14]
Acute Inflammation:
Acute inflammation typically occurs rapidly and lasts a few hours to a few days.Typical symptoms include pain, swelling, heat, redness, and loss of function. [It responds rapidly to bacterial infections, wounds, and irritants [15,16]
Chronic Inflammation:
When the stimulus continues or the inflammatory response is uncontrolled, chronic inflammation results. It lymphocytes and macrophages and frequently results in fibrosis and tissue damage. Numerous illnesses, such as cancer, asthma, chronic kidney disease, and cardiovascular disease, are linked to chronic inflammation. [17]
Acute and Chronic Pain:
Pain, both acute and chronic the nervous system recognizes and processes a variety of Environmental factors, mechanical and thermal stimuli, and As well as natural chemical irritants. Pain, both acute and chronic Are distinct clinical entities. Acute pain is linked to Sympathetic nervous system and skeletal muscle spasm When triggered by a particular illness or injury, activation serves a Beneficial biological function and is self-limiting. When deciding A chronic injury to the central and nervous systems Elements of the pain transmission pathway system Show a great deal of flexibility, intensifying pain signals and generating Hypersensitivity. This drug is frequently prescribed for Discomfort brought on by inflammation. Our body has A natural chemical system that can control pain. Brain stem, dorsal horn, and peripheral tissue fibres Release endogenous opioids and neuromodulators that prevent The way in which pain impulses are transmitted by neurons. Endorphins are naturally occurring chemicals that resemble opioids and are to alleviate pain. [18,19]
Innate Reaction:
Inflammation brought on by tissue damage and microbial infection is now understood to be a crucial component of the innate immune response. Appropriate inflammatory reactions coordinate longterm adaptive immunity against particular pathogens and offer broad protection against infections. On the other hand, persistent and unchecked inflammation frequently causes significant tissue damage, leading to significant pathogenicity from over reactive immune reactions. [20]
Adaptive Reaction:
Antigen-specific T cells must interact with activated APCs displaying cognate antigen in the context of MHC in order to successfully produce protective immunity through vaccination. The specific antigen, signal 1, and costimulatory molecule-dependent signal 2, which are necessary for complete T cell activation, are received as a result of these interactions. T cell activation requires foreign antigens introduced by vaccination to reach the secondary lymphoid organs. The lymph transports antigen to draining lymph nodes either in the form of particulates or in the form of migrating tissue-resident antigen presenting cells that have left the site of inflammation. [21,22]
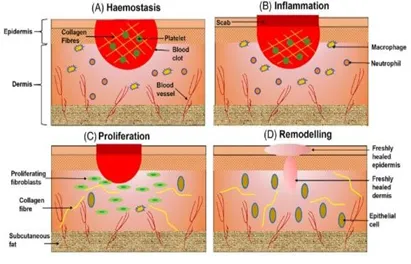
Figure 1:Schematic representation of the cutaneous wound healing
Mechanisms of action of conventional therapy
The main goals of traditional treatment for cuts and swelling are to stop the bleeding, keep the area from getting infected, ease the pain, and help the tissue heal through a number of coordinated ways. Some of the main ingredients are antiseptics, antibiotics, NSAIDs, corticosteroids, and analgesics
1. Debridement and Wound Cleaning
The process Reduces the microbial load by eliminating bacteria, necrotic tissue, and foreign particles. Stops infection and the formation of biofilms. Prepares the wound bed for healing and restores appropriate tissue perfusion.
What it does
Bacterial contamination is lessened by regular saline irrigation. Debridement accelerates healing and improves granulation tissue formation. [23]
2. Haemostasis Methods (Sutures, Pressure, Haemostatic Agents)
The process Encourages the creation of platelet plugs and vasoconstriction. Sutures reduce bleeding and restore integrity by approximating the edges of the wound.
Agents of haemostasis
Increase the formation of fibrin clots through contact activation (e.g., oxidized cellulose, gelatine sponge). [24]
3. Antiseptics (chlorhexidine and providence-iodine
The process Denature proteins, damage bacterial cell membranes, and stop enzyme activity wound colonization is prevented by broad-spectrum action.
Procedure
Reduced infection rates lead to less inflammation and quicker tissue healing. [25]
4. Antibiotics (Systemic/Topical)
The process Prevent the production of proteins or bacterial cell walls. Prevent cellulitis, abscesses, and delayed healing by lowering the bacterial burden.
Effects
Lessens inflammation brought on by bacterial toxins. Encourages the healing of wounds in a cleaner environment. [26]
5. NSAIDs (aspirin, diclofenac, ibuprofen)
The process Reduce prostaglandin synthesis by inhibiting COX-1 and COX-2 enzymes. Blocking prostaglandins lessens inflammation because they cause pain, swelling, and redness.
Herbal Therapy:
An herb is defined strictly by botany as “a seed-producing Perennial, biennial, or annual that doesn’t produce a Tent woody tissue, but it stops growing after a Season.” Naturally, customers and patients do not follothis rigorous, traditional definition when asking about out Utilising “herbal” goods. An herb can also be defined as a “plant or portion of a plant prized for its savory, medicinal, or Aromatic properties. [28]
Alovera:
Aloe was mostly classified as a member of the Lily family until recently. (Liliaceous), but Reynolds8 claims that it has since been given the Aloaceae family designation. AloeVera is a well-known wound healer and anti-inflammatory that speeds up the development of epithelial tissue. [23]
Aloe Vera’s mechanism of action for wounds. According to reports, healing increases the turnover rate of collages and Elevated lysis oxidase level, which is in charge of cross-linking Collages that have recently been synthesized (Chitra et al., 1998). [29]
Pharmacological Effect of Alovera Gel:
Burn and Wound Healing Property: The main benefits of aloe Vera are its calming and restorative properties. Consequences for burns and other injuries. Aloe Vera’s ability to reduce inflammation and Analgesic effects in animal models used in experiments. Aloe Vera, also known as Aloe barbadensis
Miller, is a member of the Family Liliaceae. The succulent plant aloe Vera Grows in a hot, environment. [30] Cosmetics and some medication The mucilaginous tissue in the product is used to make Aloe Vera gel is the substance found in the centre of aloe Vera leaves. The Aloe Vera’s peripheral bundle sheath cells generate Highly bitter, yellow latex, often known as aloe that Possesses laxative properties. Nevertheless, whole leaf extracts might Have anthraquinones in them. Examined the effects of pharmacology Of aloe in animals or in vitro, such as anti- Antibacterial, anti-inflammatory, and antiarthritic properties And effects on hypoglycaemia. The use of aloe Vera has included for millennia in a number of cultures for therapeutic purposes. There are 75 potentially active components in aloe Vera: Minerals, sugars, lignin, spooning, vitamins, enzymes, Amino acids and salicylic acids.
Antioxidant: vera enhances the Blood quality, most likely by enabling the blood to. Efficiently deliver nutrients and oxygen to the cells Body.[31,32]
Preparation of lotion containing beads and aloe gel:
Novel lotion was prepared by suspending equivalent to 2gm aloe gel beads in 15ml of calamine lotion BP. The conventional lotion was prepared by incorporating the 2gm aloe gel directly into 15ml. [27]
Included in vitro studies are frequently Used Student’s t-test and ANOVA to analyse experimental Information. [33,34]

Figure 2:Aloe gel beads
Herbs used in laceration And Inflammation
|
Herb |
Active compounds |
Actions |
Evidence |
|
Curcuma longa |
Car cumin |
Anti-inflammatory anti-oxidant |
Nano formulation 30% faster healing [35,36] |
|
Neem |
Nimbi din, Nimbolide |
Antimicrobial, inflammatory |
Animal studies: Decrease bacterial load increase contraction [37] |
|
Tulsi |
Eugenol ursolic acid |
Anti-Inflammatory Collagen synthesis |
Rat wound:35% epithelialization [38] |
|
Moringa |
Vitamins polyphenols |
Antioxidant, fibroblasts stimulation |
Animal: Increasetensile strength, Decrease Wound Area [39] |
Mechanisms of Herbal Therapy:
Wound + Inflammation + General
Herbal therapy works because plants contain bioactive compounds such as flavonoids, tannins, Alkaloid saponins, terpenoids, phenolic acids, essential oils, and most of These drugs affect the body in a number of ways, such as: Controlling the Inflammatory Process.
Specific Mechanism
A number of herbal components inhibit the production of pro-inflammatory mediators like prostaglandins and leukotrienes by blocking the activity of the cyclooxygenase (COX-2) and lipoxygenase (LOX) enzymes. Certain phytochemicals disrupt the NF-κB signalling cascade, a crucial pathway that inflammatory cytokines like TNF-α, IL-1β, and IL-6. Herbs help stop additional tissue damage and swelling by lowering the activation of neutrophils and macrophages. [40]
1. Reduction of Oxidative Stress and Antioxidant Defence:
After a cut, the damaged tissue generates a lot of free radicals.
Specific Mechanism
Herbal compounds high in phenolic acids and flavonoids neutralize unstable free radicals by giving them electrons. This antioxidant activity shields endothelial cells, fibroblasts, and keratinocytes from oxidative damage. Herbs aid in preserving the integrity of the cell membranes surrounding the wound by inhibiting lipid peroxidation. [41]
2. Fibroblast Activity and Collagen Production Increased Fibroblast Activity and Collagen
Production
Increased Fibroblast Activity and Collagen Production Collagen synthesis plays a major role in the proliferative stage of wound healing.
Specific Mechanism
Numerous herbal extracts promote fibroblast growth, which facilitates the quick deposition of collagen Types I and III. Certain substances stimulate growth factors such as TGF-β and VEGF, whic encourage the production of extracellular matrix and angiogenesis. Tensile strength is increased and the tissue is strengthened by better collagen cross-linking. [42]
3. Early Wound Phases of Haemostatic Activity
Certain herbs have inherent blood-clotting qualities that can be applied right away following a cut.
Specific Mechanism
Platelet aggregation is encouraged by bioactive tannins and polysaccharides. Vasoconstriction brought on by astringent substances lowers blood flow to the injured area. The wound is stabilized and contamination is avoided with quicker fibrin clot formation. [43]
Why Herbal Remedies Are Usually Effective
Herbal remedies are highly effective in treating both cuts and inflammation due to these combined biological effects.
There are several applications for herbal therapy. It operates using several strategies:
FUTURE PROSPECTS
To promote quicker and Safer wound healing standardized Herbal Formulation combine to in the future to treat inflammation and laceration. The delivery and efficacy Of herbal active can be enhanced by cutting edge technology Like hydrogels nanoparticles.
CONCLUSION
This review successfully contrasts herbal and conventional methods for treating inflammation and cuts. Conventional therapies concentrate on using sutures or staples to close wounds and NSAIDs and antiseptics to reduce pain and swelling. Using bioactive substances from plants like aloe Vera, curcuma longa, neem, and Tulsi, herbal therapy offers a promising substitute. These herbs fight infection, lower inflammation, provide antioxidant protection, and speed up wound healing by increasing the production of collagen. In the end, the results point to an integrated management approach in which standardized herbal formulations—possibly administered through cutting-edge technologies like hydrogels—can successfully supplement traditional care for safer and faster tissue repair.
REFERENCES






Deshna Khartad, Roshani Kale, Maithili Kalbande, Rupeshri Netkar*, Vaishnavi Gole, Prashil Dhumale, Pranali Bhande, A Review on Laceration and Inflammation Management by Conventional and Herbal Therapy, Int. J. Med. Pharm. Sci., 2026, 2 (7), 349-357. https://doi.org/10.5281/zenodo.21245010
 10.5281/zenodo.21245010
10.5281/zenodo.21245010